
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


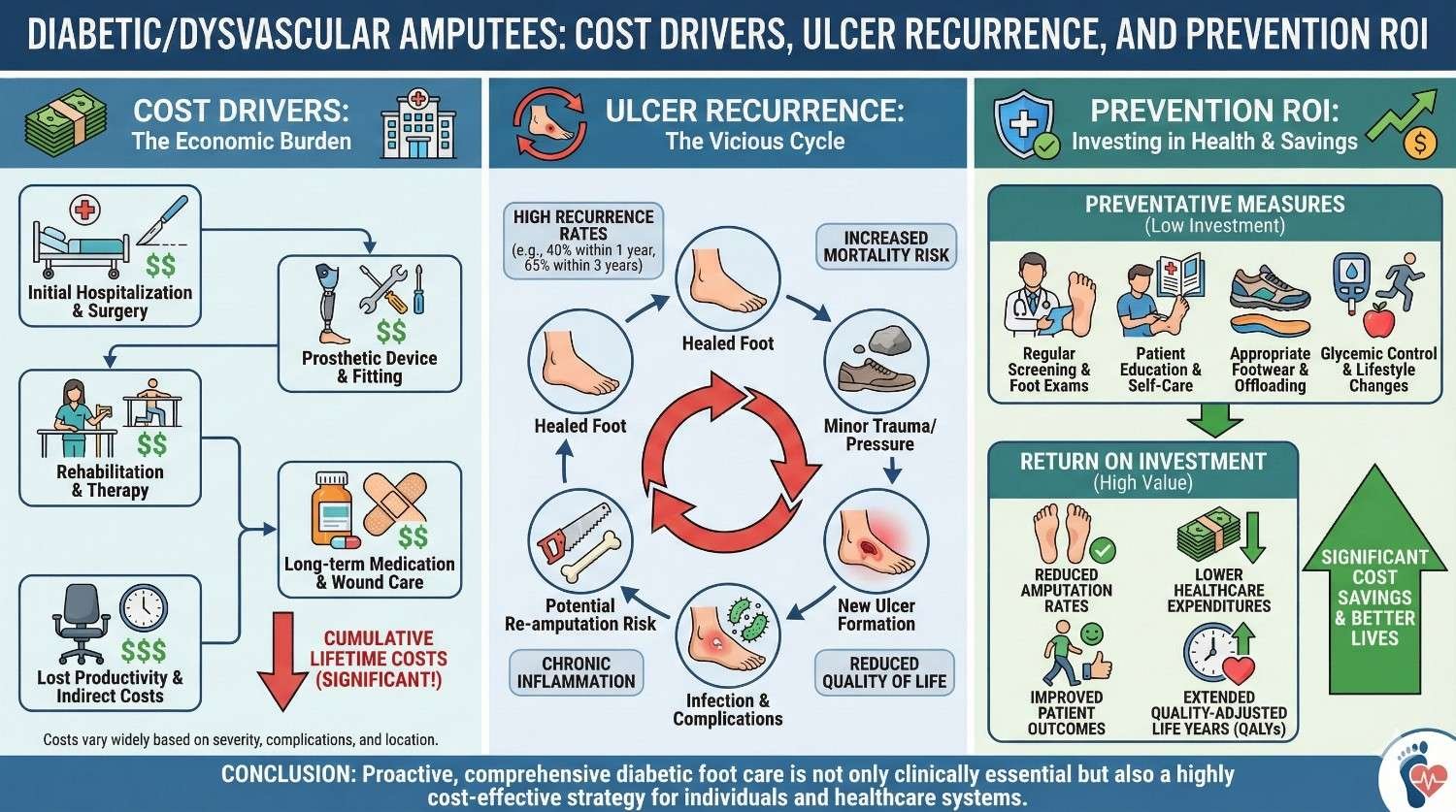
Diabetic and dysvascular amputations are not sudden events. They are the result of a long chain of missed prevention, delayed care, and fragile healing. For hospitals and care teams, the real challenge begins after surgery, when the risk of ulcer return, infection, and readmission stays high for years.
This article looks closely at the true cost drivers in diabetic and dysvascular amputee care. We will explore why ulcers come back, how prosthetic and follow-up choices affect outcomes, and where prevention delivers the strongest return on investment. The focus is practical, honest, and grounded in real care settings, with one clear goal. Fewer ulcers, fewer admissions, and better long-term value for both patients and health systems.
In trauma-related amputations, the injury is usually a one-time event. In diabetic and dysvascular cases, the disease that caused the amputation is still active. Poor circulation, nerve damage, and slow healing do not stop after surgery.
This means the limb that remains, and even the residual limb, continue to face risk. Pressure, friction, or a small wound can quickly turn into a serious ulcer. Cost planning that treats these patients like standard amputees almost always fails.
Many diabetic patients have reduced or absent sensation. They cannot feel early pain or pressure the way others can. This removes a natural warning system.
A poorly fitting socket, a wrinkle in the liner, or excess heat may go unnoticed for days. By the time the problem is visible, the damage is already deep. This delayed detection is a major cost driver.
Blood flow in dysvascular patients is often limited. Even minor skin breaks take longer to heal. Infection spreads faster when circulation is poor.
This fragile healing environment means that small prosthetic issues carry high financial risk. Prevention is not optional. It is essential.
Ulcers are not one-time events. Once a diabetic amputee develops an ulcer, the chance of recurrence is high. Each recurrence increases the risk of infection, hospitalization, and further limb loss.
Every ulcer episode triggers a cascade of costs. Wound care visits, imaging, antibiotics, possible surgery, and often prosthetic downtime. Over time, these episodes far outweigh the initial prosthetic cost.
Diabetic amputees are frequently readmitted for wound-related issues. These stays are often longer than average due to slow healing and infection risk.
Extended stays increase direct hospital cost and strain bed capacity. They also attract penalties in many reimbursement models.
Reducing readmissions is one of the clearest financial opportunities in this group.
When ulcers recur, patients often stop using their prosthesis. This leads to reduced mobility, weight gain, and decline in overall health.
Prosthetic abandonment increases dependence on care services and raises long-term cost. It also wastes the original prosthetic investment.
Keeping patients safely ambulatory is both a clinical and financial priority.
Diabetic residual limbs often have uneven tissue, scars, and fragile skin. Even well-designed sockets can create pressure points over time.
As limb volume changes, pressure shifts. Without regular monitoring, these shifts lead to breakdown.
Ulcer prevention requires constant attention, not a one-time fitting.
Many patients walk barefoot at home. Some use worn-out footwear. Others ignore early signs because they do not feel pain.
These habits are often driven by lack of education rather than neglect. Addressing behavior is part of prevention.
After initial rehabilitation, follow-up often becomes irregular. Transportation challenges, cost concerns, and lack of awareness all play a role.
Without consistent follow-up, small problems grow into major ones.
Regular contact is one of the most effective ulcer prevention tools.
For diabetic amputees, socket fit is not about comfort alone. It is about skin survival.
Even minor misalignment can create shear forces that break fragile skin. A socket that works for months can become unsafe as limb volume changes.
Regular reassessment of fit is essential to prevent breakdown.
Some materials trap heat and moisture. In diabetic patients, this creates a perfect environment for skin damage and infection.
Breathable liners, moisture control, and easy inspection features reduce risk. These choices may cost more upfront but save much more later.
Unstable gait increases fall risk and creates abnormal loading patterns. These patterns increase pressure in areas not designed to bear it.
Prosthetic stability supports even weight distribution, reducing stress on vulnerable skin.

Most ulcers start small. Redness. Warmth. Slight swelling.
Without follow-up, these signs are missed. Patients often present only when the wound is open and infected.
Early visits are cheaper than late admissions.
When problems escalate, care becomes urgent. Emergency visits, hospital admission, and aggressive treatment follow.
These episodes cost many times more than routine preventive care.
Preventive follow-up is one of the highest return investments in this population.
Repeated admissions for the same issues frustrate clinicians and nurses. It creates a sense of failure and fatigue.
Better prevention improves morale and care quality.
Traditional care models react to ulcers. Prevention-focused models aim to stop them from forming.
This shift changes spending patterns. Money moves from emergency care to planned care.
Planned care is almost always cheaper and more effective.
Simple actions like scheduled socket checks, patient education, and timely liner replacement reduce ulcer risk significantly.
These interventions are low cost compared to the expense of wound care and hospitalization.
The return on investment is clear and measurable.
Ulcer prevention supports prosthetic use, mobility, and independence. These outcomes reduce downstream cost across multiple systems.
Prevention is not a single action. It is a strategy that protects everything built around it.
Cost alone does not tell the full story. Ulcer-free days, prosthetic wear time, and patient mobility are important indicators.
These measures show whether prevention is working.
When ulcers decrease, costs follow.
Hospitals often underestimate how much they spend on ulcer treatment because costs are spread across departments.
When these costs are added together, prevention programs often pay for themselves many times over.
Clear comparisons strengthen the case for investment.
Tracking ulcer rates, readmissions, and follow-up adherence creates accountability.
Data turns prevention from a belief into a proven strategy.
Hospitals should not leave follow-up to chance. Clear schedules, reminders, and defined responsibilities improve consistency.
Structured pathways reduce gaps that lead to ulcers.
Prosthetic care cannot exist in isolation. Coordination with diabetes management, vascular care, and wound specialists is critical.
Integrated care reduces duplication and improves outcomes.
Prevention requires a mindset shift. Teams must be trained to look for risk before damage appears.
This proactive approach saves time, money, and lives.
Simple daily inspection routines help patients catch problems early. Education must be repeated and reinforced.
Visual aids and hands-on training improve understanding.
Empowered patients reduce emergency visits.
Education must fit the patient’s life. Advice that ignores living conditions or habits is rarely followed.
Practical guidance works better than ideal instructions.
Prevention is a habit, not a one-time lesson. Regular reinforcement builds lasting behavior change.
Habit change protects health and budgets.
When budgets are tight, follow-up visits are often reduced. This creates short-term savings but long-term loss.
Ulcers return. Admissions rise. Total cost increases.
Cutting prevention is false economy.
Low-cost prosthetic components may lack features that protect skin and stability. In diabetic patients, this risk is magnified.
Upfront savings often lead to higher downstream cost.
Education is sometimes seen as optional. In reality, it is one of the cheapest and most effective interventions available.
Ignoring it increases risk significantly.
The evidence is clear. Prevention reduces ulcers, admissions, and cost.
Hospitals that adopt preventive prosthetic models lead in both outcomes and efficiency.
Healthcare payment models increasingly reward prevention and penalize avoidable complications.
Ulcer prevention aligns strongly with these trends.
Fewer ulcers mean less pain, fewer surgeries, and better quality of life.
They also mean stronger hospitals and more sustainable care systems.

Ulcer prevention does not begin when the prosthesis is delivered. It starts much earlier, during wound healing and limb shaping.
Residual limbs that heal with uneven scars, excess swelling, or poor skin condition are more likely to break down later. Early coordination between surgeons, wound teams, and prosthetists reduces long-term risk.
Hospitals that invest time at this stage often see fewer complications months later.
Not all diabetic amputees carry the same level of risk. Some have better circulation, stronger family support, and good disease control. Others face multiple challenges at once.
Effective programs stratify patients by risk and match follow-up intensity accordingly. High-risk patients need closer monitoring and more frequent adjustments.
This targeted approach improves outcomes without overusing resources.
Follow-up should be treated as part of treatment, not an optional add-on. Missed visits often precede ulcer recurrence.
Hospitals that build follow-up into care pathways, with reminders and clear accountability, reduce dropouts.
Consistency is more powerful than complexity.
Diabetic residual limbs need sockets that spread pressure evenly and reduce shear. Sharp pressure points and rigid edges increase breakdown risk.
Design choices such as total contact sockets, soft interfaces, and adjustable features help protect skin as limb shape changes.
These design decisions often cost little more but deliver major protection.
Heat and moisture weaken skin. In diabetic patients, this effect is amplified.
Breathable liners, moisture-wicking materials, and easy-to-clean interfaces reduce skin stress. They also encourage regular inspection, which helps catch problems early.
Comfort supports compliance, and compliance protects skin.
A stable prosthesis reduces uneven loading and sudden shifts in pressure. This lowers the risk of skin injury.
Advanced feet and knees that support smoother walking reduce abnormal forces on the residual limb.
Stability is not a luxury. It is a preventive feature.
Advanced prosthetic components often face resistance due to higher initial cost. This view ignores lifetime expense.
When better components reduce ulcers, hospitalizations, and prosthetic abandonment, they lower total cost over time.
Hospitals that look beyond purchase price make better financial decisions.
Reliable components fail less often. Fewer failures mean fewer emergency visits and fewer care disruptions.
Predictability reduces cost and stress for both patients and providers.
Reliability is an economic advantage.
Not every patient needs the most advanced solution. High-risk patients benefit most from protective features.
Stratified device selection improves ROI by matching investment to need.

Ulcer prevention works best when it is integrated. Prosthetic design alone is not enough. Education alone is not enough.
Programs that combine good fitting, regular review, and patient education achieve the strongest results.
Integration reduces duplication and gaps.
Effective programs rely on simple, repeatable actions. Routine skin checks. Scheduled socket reviews. Clear escalation steps.
Complex protocols often fail in busy clinics. Simple ones survive.
Consistency delivers results.
Tracking ulcer recurrence, readmissions, and prosthetic use provides clear evidence of impact.
When teams see results, motivation increases. When leaders see data, support grows.
Measurement sustains programs.
Ulcers are late signs. Teams must be trained to spot early risk signals such as gait changes, limb volume shifts, and patient fatigue.
Early intervention is cheaper and safer.
Training builds a preventive culture.
Prosthetists, nurses, doctors, and therapists often work in parallel. Ulcer prevention requires them to work together.
Shared notes and regular case discussions reduce missed signals.
Communication saves limbs and money.
Repeated ulcer cases can demoralize teams. Prevention reduces this cycle.
When teams see patients staying healthy, job satisfaction improves.
Healthy teams deliver better care.
Telling patients what to do is not enough. Prevention works when patients feel involved and respected.
Listening to daily challenges helps tailor advice that patients can follow.
Partnership builds trust and adherence.
Daily inspection should fit into the patient’s routine. Complicated instructions are often ignored.
Simple, repeatable habits work best.
Small actions done daily prevent big problems.
Education fades if not reinforced. Regular reminders during visits strengthen habits.
Repetition saves skin.

Ulcers increase the risk of higher-level amputation. Each additional amputation multiplies cost and reduces quality of life.
Prevention protects the remaining limb and the patient’s future.
This is one of the highest-value outcomes possible.
Patients who avoid ulcers stay mobile. Mobility supports work, family roles, and mental health.
These benefits reduce reliance on healthcare and social support systems.
Prevention creates value far beyond clinics.
When ulcer rates fall, pressure on beds, staff, and budgets reduces.
Systems become more resilient and sustainable.
Prevention strengthens the whole system.
Prevention programs often struggle because benefits appear over time, not immediately.
Leadership commitment is needed to look beyond quarterly cycles.
Long-term thinking pays off.
When no one owns prevention, it fails. Clear ownership improves execution.
Assigning responsibility creates accountability.
Social, economic, and cultural factors affect prevention. Programs must adapt to reality, not ideals.
Understanding context improves success.

Ulcer prevention should be part of standard amputee care, not a separate initiative.
Embedding it into routine practice ensures consistency.
Standard care delivers standard results.
Prevention aligns with goals of quality, safety, and cost control.
It is not an extra burden. It is a strategic advantage.
Hospitals that lead in prevention protect patients and resources at the same time.
This leadership matters.
Diabetic and dysvascular amputee care is complex, but the pattern is clear. Ulcers drive cost. Prevention protects value.
Small, consistent actions reduce recurrence, admissions, and long-term harm. The return on investment is not theoretical. It is visible in fewer wounds, fewer hospital stays, and stronger patient trust.
When prevention becomes the norm, everyone benefits. Patients heal better. Teams work with confidence. Systems grow stronger.
That is the real return on investing in ulcer prevention.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body