
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Limb salvage is often chosen with hope, patience, and the desire to preserve what remains, but there are times when continued salvage causes more harm than benefit. For doctors, the hardest part is knowing when to pause, reassess, and consider prosthetic referral without feeling that care has failed. This decision is not about giving up; it is about protecting life, function, and dignity.
This article explores the clinical triggers that signal limb salvage failure and the right time to discuss prosthetic referral. It is written for MDs who manage complex wounds, repeated surgeries, chronic infection, and long rehabilitation journeys. The focus is on clear medical signs, functional outcomes, and patient well-being, so that decisions are timely, ethical, and patient-centered.
Limb salvage is chosen to preserve anatomy, maintain sensation, and avoid the emotional impact of amputation, especially in younger or medically complex patients.
It often involves multiple surgeries, long wound care, and extended rehabilitation, all with the hope of restoring useful function.
Understanding this goal is important before defining when salvage stops being beneficial.
In many cases, limb salvage extends over months or even years, with repeated hospital visits and slow progress.
What begins as a reasonable attempt can quietly turn into a cycle of procedures with limited functional gain.
Doctors must recognize when duration itself becomes a clinical concern.
High surgical effort does not always translate into meaningful recovery.
A salvaged limb that cannot bear weight, tolerate load, or support daily activity may still limit independence.
Outcome, not intent, should guide next steps.
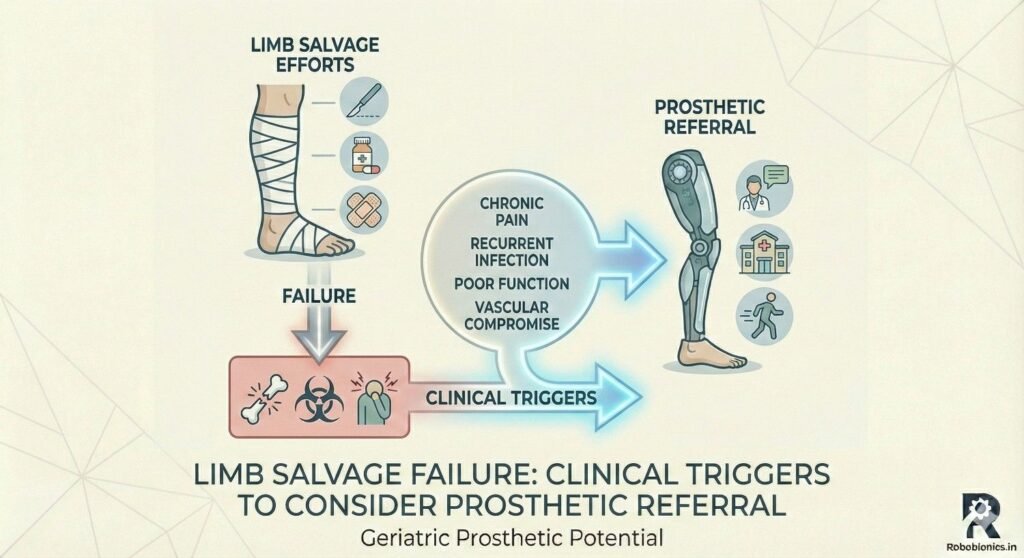
Poor circulation reduces oxygen delivery and limits the body’s ability to heal despite optimal surgical technique.
Repeated failure of wounds to granulate or close often signals that vascular limits have been reached.
At this stage, continued salvage may increase infection risk without improving function.
Persistent infection that returns after debridement and antibiotics is a strong warning sign.
Biofilms protect bacteria and make eradication difficult even with aggressive care.
Ongoing infection increases pain, fatigue, and systemic risk.
Repeated surgeries and inflammation weaken skin, muscle, and bone.
Over time, tissue becomes less tolerant of reconstruction or load.
This gradual decline is often subtle but clinically significant.
When surgeries become more frequent without proportional improvement, it suggests diminishing returns.
Each procedure carries anesthesia risk, healing delay, and emotional strain.
Doctors should pause and reassess after repeated interventions.
Progression from simple closure to flaps, grafts, or staged reconstructions often reflects worsening tissue conditions.
While these techniques are valuable, their repeated need may signal that salvage is struggling biologically.
Complexity alone is not failure, but escalation without progress is concerning.
When remaining options are limited or high risk, the margin for safe salvage narrows.
At this point, planning for prosthetic referral becomes part of responsible care.
Early discussion prevents crisis decisions later.
A limb that cannot safely accept weight after prolonged treatment limits mobility and independence.
Repeated offloading, bracing, or non-weight-bearing instructions often reduce quality of life.
Function should be evaluated honestly, not optimistically.
Reliance on walkers, crutches, or wheelchairs long term may indicate limited salvage benefit.
While aids are useful, permanent dependence after extensive salvage suggests restricted functional return.
This pattern should prompt reassessment.
Chronic pain that persists despite healing attempts affects sleep, mood, and participation.
Pain-driven avoidance often reduces strength and balance further.
Uncontrolled pain is a major trigger for reconsidering goals.
Wounds that reopen repeatedly despite care indicate poor tissue resilience.
Each breakdown increases infection risk and patient frustration.
This pattern is a clear clinical signal.
Healing that stretches far beyond expected timelines suggests systemic or local failure.
Prolonged open wounds affect nutrition, mobility, and mental health.
Delayed closure should always prompt broader discussion.
Long-term reliance on negative pressure therapy, dressings, or frequent debridement may signal limited progress.
While these tools support healing, indefinite use raises questions about endpoint.
Doctors should evaluate whether the plan is moving forward or standing still.
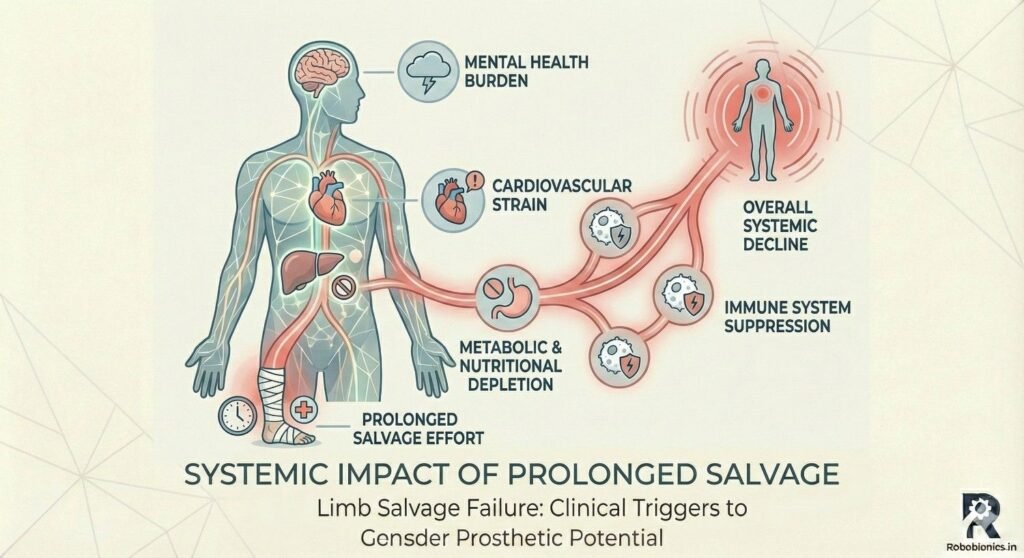
Extended immobility and repeated infections can weaken cardiovascular and respiratory health.
Patients may lose muscle mass and endurance over time.
This decline affects future rehabilitation potential.
Chronic wounds increase metabolic demand.
Poor nutrition slows healing and reduces strength.
Fatigue becomes both a symptom and a barrier.
Long salvage journeys often lead to emotional burnout.
Patients may lose hope or trust in the process.
Mental fatigue should be taken seriously as a clinical factor.
Statements like “this will never heal” or “I am tired of surgeries” often reflect deep distress.
These words are clinical data, not complaints.
They should trigger careful conversation.
Missed appointments or reduced engagement may indicate emotional overload.
This behavior often appears before physical decline becomes obvious.
Early recognition allows supportive intervention.
When patients ask about amputation or prosthetics, it often follows long reflection.
This question deserves respect and honest discussion.
Ignoring it can damage trust.
A poorly functioning salvaged limb may limit mobility more than a well-fitted prosthesis.
Doctors should compare realistic outcomes, not ideal ones.
This comparison must be grounded in daily life needs.
Salvaged limbs that require braces or altered gait often increase energy use.
Prosthetic walking may sometimes be more efficient.
Efficiency matters for long-term health.
Prosthetic rehabilitation often follows a clearer timeline than prolonged salvage.
Predictability helps patients plan life and work.
This factor influences quality of life.
Late referral after physical decline can reduce prosthetic success.
Timely discussion preserves rehabilitation potential.
Delay can unintentionally limit future options.
Doctors should present prosthetic referral as a medical option, not a failure.
Patients deserve clear information about risks and benefits.
Shared decisions build trust.
Quality of life and independence matter as much as limb preservation.
Ethical care respects dignity over anatomy.
This principle should guide referrals.
Language should focus on function, comfort, and future potential.
Avoid framing amputation as defeat.
Clear framing reduces fear.
Many patients fear prosthetics due to misconceptions.
Early education helps reset expectations.
Accurate information empowers choice.
Early referral does not commit the patient to amputation.
It allows assessment and planning.
This approach reduces pressure later.
Both aim to restore function and dignity.
They are parts of the same continuum of care.
Understanding this reduces emotional resistance.
The same decision made earlier or later can lead to very different results.
Recognizing triggers early protects options.
Timing is a core clinical skill.
Doctors help patients navigate uncertainty and change.
Guidance requires honesty, compassion, and courage.
This role shapes long-term outcomes.
We have now covered the key clinical triggers and decision points that indicate when limb salvage may be failing and when prosthetic referral should be considered.
Some patients experience repeated fractures, soft tissue loss, or implant failure in the same limb, where each new injury compounds existing damage and reduces the chance of meaningful recovery.
Over time, healing slows, pain increases, and functional milestones move further away rather than closer.
This pattern often signals that the limb is no longer biologically or mechanically resilient enough for salvage.
Patients with open fractures or contaminated wounds may experience cycles of infection that respond briefly to treatment and then return.
Each recurrence weakens tissue quality and increases systemic risk.
When infection becomes a repeating pattern rather than a one-time event, prosthetic referral should enter the discussion.
When flap surgeries, grafts, or bone reconstructions repeatedly fail or provide only short-lived improvement, the likelihood of durable salvage decreases.
The limb may appear intact but remain painful, unstable, or nonfunctional.
Doctors should recognize this pattern early to prevent prolonged suffering.
A limb may be surgically preserved yet unable to support standing, walking, or basic daily tasks.
This mismatch between appearance and function often leads to frustration and dependence.
Functional outcome should carry more weight than radiological or surgical success alone.
When patients cannot return to work, self-care, or community mobility despite prolonged salvage efforts, the benefit of continued treatment must be questioned.
Extended inactivity often leads to muscle loss, social isolation, and mental decline.
Prosthetic referral may offer a clearer path back to participation.
Growing dependence on family or caregivers for basic mobility and hygiene is a strong signal that current treatment is not restoring independence.
This dependence affects both patient dignity and family burden.
Restoring autonomy should be a core clinical goal.
Frequent admissions for wound care, infection control, or revision surgery disrupt normal life and strain health systems.
These interruptions often erode patient morale and physical conditioning.
Cumulative burden should factor into decision-making.
Extended time away from work or school affects financial stability and self-identity.
Delayed functional recovery often deepens these losses.
Earlier prosthetic planning may reduce long-term socioeconomic impact.
Patients undergoing years of salvage may feel emotionally and physically exhausted.
Burnout reduces adherence and healing potential.
Recognizing fatigue early allows for more compassionate care choices.
Salvage often carries uncertain timelines with frequent setbacks.
Prosthetic rehabilitation, while challenging, usually follows clearer stages.
Predictability helps patients regain control over planning their lives.
Prolonged non-weight-bearing or altered gait can damage the spine, hips, and opposite limb.
Prosthetic walking may distribute load more evenly over time.
Long-term health should influence referral timing.
Living without clear endpoints can be emotionally draining.
A defined prosthetic pathway may reduce anxiety and restore hope.
Mental well-being is a valid clinical outcome.
Early mention of prosthetic options prepares patients emotionally without forcing a decision.
This approach reduces shock if salvage later fails.
Early awareness preserves trust.
Discussing mobility, comfort, and daily life resonates more than technical details.
Patients relate better to function than anatomy.
Clear language supports shared understanding.
Patients need time to process the idea of change.
Rushed discussions increase resistance.
Respecting pacing improves acceptance.
Stabilizing infection, nutrition, and general health improves prosthetic outcomes.
Early optimization preserves future rehabilitation potential.
Referral should be planned, not reactive.
Early involvement of rehab specialists helps set realistic expectations.
This coordination smooths transition if amputation becomes necessary.
Team-based planning improves outcomes.
Clear documentation of salvage history helps prosthetic teams plan effectively.
Continuity prevents repetition of unsuccessful approaches.
Shared records support patient-centered care.
Sudden increase in pain, swelling, or infection may indicate imminent failure.
Delayed action in such cases increases risk.
Urgent reassessment is essential.
Fever, weight loss, or repeated sepsis episodes suggest that the limb is affecting overall health.
At this stage, limb preservation may threaten life.
Prosthetic referral becomes a protective measure.
When patients lose confidence in the care plan, adherence drops.
Trust erosion often precedes medical decline.
Restoring trust may require changing direction.
Prosthetic assessment can occur alongside salvage efforts without committing to amputation.
This parallel approach keeps options open.
Early planning reduces crisis decisions.
Many patients hold outdated views of prosthetic function.
Education can shift fear into informed consideration.
Knowledge empowers choice.
Families often influence major decisions.
Including them early reduces conflict and misunderstanding.
Shared understanding improves support.
At Robobionics, we have worked with many patients whose journeys began with limb salvage and eventually moved toward prosthetic rehabilitation, and one pattern is clear: timely referral is not a sign of failure, but a sign of clinical maturity and patient-centered thinking.
When salvage no longer restores comfort, function, or dignity, changing direction protects long-term health and independence.
Doctors play a critical role in helping patients see this transition as a step forward rather than an end.
We have seen that patients cope better when prosthetic options are discussed early, even while salvage is ongoing, because it removes fear of the unknown and allows emotional preparation.
Honest conversations grounded in function, safety, and daily life outcomes build trust and reduce resistance.
These discussions give patients back a sense of control during uncertain times.
Delayed referral after prolonged infection, immobility, or systemic decline often limits what prosthetic rehabilitation can achieve.
When referral happens while the patient still has strength, motivation, and medical stability, outcomes are consistently better.
Timing, more than technology, defines success.
Surgeons, physicians, wound care teams, and prosthetic providers all work toward the same goal: restoring meaningful life participation.
Limb salvage and prosthetics are not opposing philosophies but connected paths within the same continuum of care.
Strong collaboration ensures that patients are not trapped between options but guided through them.
As an Indian prosthetics manufacturer, Robobionics designs and delivers solutions that are affordable, serviceable, and suited to real-world clinical and social conditions.
We work closely with doctors to support early assessment, patient education, and smooth transition when prosthetic referral becomes the right choice.
Our aim is to help clinicians restore mobility with dignity, clarity, and long-term confidence.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body