
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


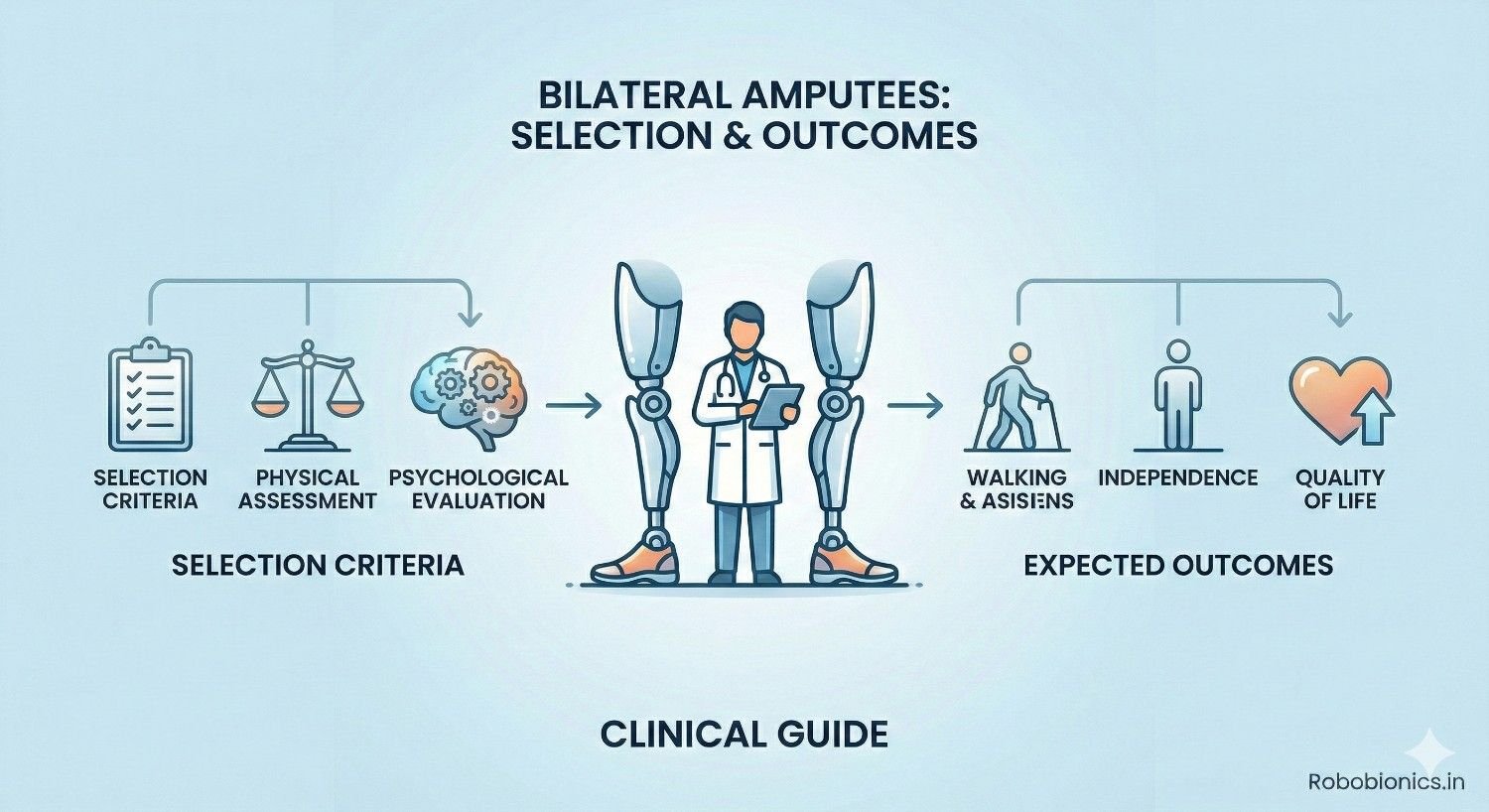
Bilateral amputation changes movement, balance, and independence in ways that go far beyond losing a single limb. For clinicians, selecting the right candidates for bilateral prosthetic rehabilitation requires careful judgment, realistic goal setting, and a deep understanding of both physical and psychological demands. The decisions made early often shape whether a patient regains mobility or faces long-term dependence.
This article explores selection criteria and expected outcomes for bilateral amputees in a clear and practical way, designed for doctors working in real clinical settings. It focuses on medical readiness, functional potential, emotional strength, and social support, helping clinicians decide who will benefit most from bilateral prosthetics and what outcomes can reasonably be expected over time.
Bilateral amputees face the loss of symmetry, balance, and natural load sharing, which makes movement more demanding and energy intensive than in unilateral cases.
Every task, from standing up to walking a few steps, requires higher coordination and strength.
Clinicians must view bilateral rehabilitation as a separate pathway, not an extension of unilateral care.
Bilateral amputation often results from vascular disease, diabetes, severe trauma, infection, or complications following limb salvage.
These underlying causes usually affect overall health, not just the limbs.
Selection criteria must therefore consider systemic disease alongside local limb status.
Some bilateral amputees regain high levels of independence, while others remain limited despite good devices.
Differences in health, motivation, and support explain much of this variation.
Early assessment helps predict which path is more likely.
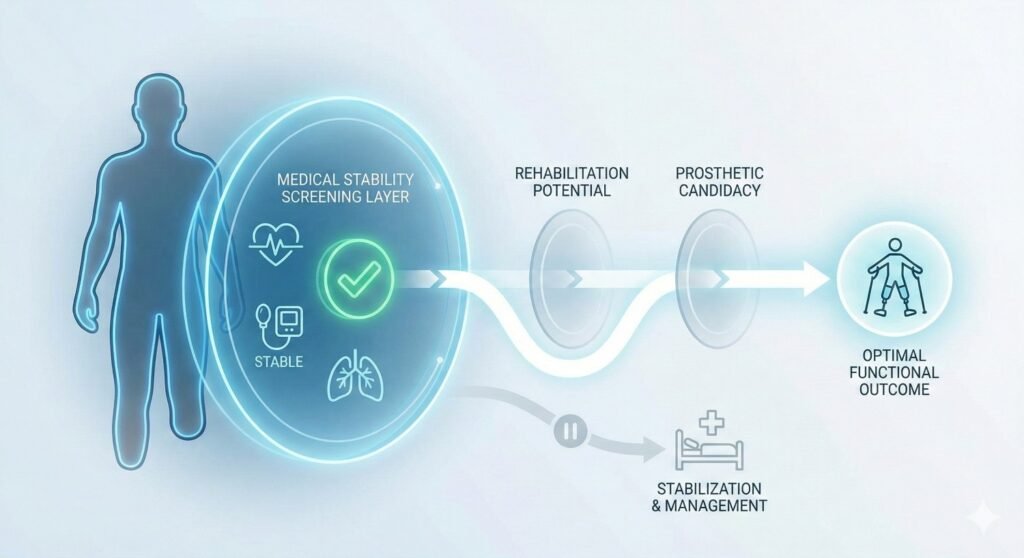
Bilateral prosthetic walking demands significantly more energy than unilateral walking.
Patients with limited heart or lung reserve may fatigue quickly and face safety risks.
Medical clearance should focus on endurance, not just wound healing.
Conditions such as diabetes and kidney disease affect healing and strength.
Stable medical control supports safer rehabilitation and fewer setbacks.
Unstable disease often limits achievable outcomes.
Active or recurrent infection anywhere in the body increases rehabilitation risk.
Bilateral amputees have less margin for medical instability.
Infection control is essential before prosthetic trials.
Both residual limbs must tolerate socket pressure and shear.
Fragile skin on even one side can limit bilateral use.
Clinicians should assess tolerance over time, not at a single visit.
Short or uneven limb lengths increase energy cost and balance difficulty.
Muscle strength and control around both stumps influence stability.
These factors shape device choice and expectations.
Persistent pain or hypersensitivity can limit training intensity.
Pain on both sides compounds difficulty.
Pain control is a prerequisite for progress.
Without natural limbs for balance correction, trunk stability becomes critical.
Weak core muscles increase fall risk.
Pre-prosthetic conditioning is often necessary.
Upper limbs support transfers, mobility aids, and early walking.
Weak arms limit independence.
Strength testing should be part of selection.
Ability to maintain balance with support provides insight into potential.
Severe instability predicts slower progress.
Early balance testing guides goal setting.
Bilateral prosthetic use requires learning new movement strategies.
Patients must process feedback and adjust continuously.
Cognitive readiness affects training speed and safety.
Training involves repeated instruction and correction.
Poor memory or focus slows learning.
Clinicians should screen for cognitive barriers.
Falls carry higher consequences for bilateral users.
Good judgment and risk awareness are essential.
Poor insight increases danger.
Bilateral loss often triggers deeper grief and fear than unilateral loss.
Patients may feel a greater sense of dependency.
Emotional screening is critical.
Some patients feel forced to pursue prosthetics due to family or social expectations.
Externally driven motivation often fades.
Internal motivation predicts better outcomes.
Bilateral rehabilitation progresses gradually.
Patients who accept slow gains adapt better.
Impatience leads to frustration.
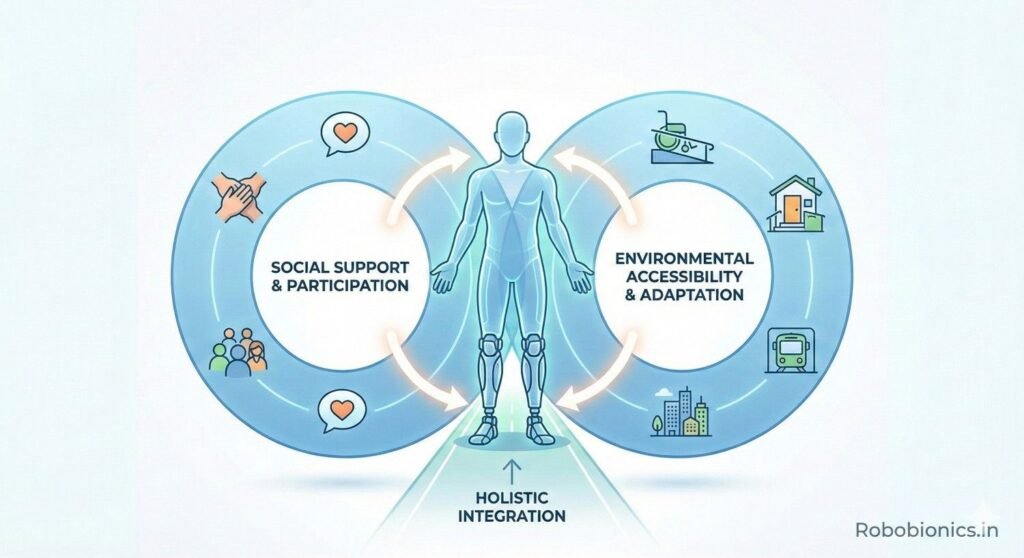
Steps, narrow spaces, and uneven floors affect safety.
Environmental barriers may limit prosthetic use.
Home assessment informs realistic goals.
Daily assistance is often needed in early stages.
Supportive caregivers improve outcomes.
Lack of support increases risk.
Return-to-work expectations influence goal setting.
Not all jobs suit bilateral prosthetic use.
Counseling may be needed.
Small alignment errors are magnified in bilateral users.
Precise fitting is essential.
Regular review is required.
Heavier devices increase fatigue.
Lightweight designs improve tolerance.
Component choice affects outcomes.
Complex systems require higher learning capacity.
Simpler solutions may work better initially.
Progression can be staged.
Many bilateral amputees achieve safe indoor walking.
Outdoor mobility may be limited or aided.
Goals should match capacity.
Walkers or canes may remain part of mobility.
Using aids does not mean failure.
Safety takes priority.
Transfers, self-care, and short walks define success.
Complete independence is not universal.
Clinicians should redefine success.
Bilateral rehabilitation takes more time.
Patients should expect extended therapy.
Clear timelines reduce frustration.
Progress often comes in phases.
Plateaus are normal.
Reassurance helps persistence.
Ongoing review prevents complications.
Adjustment is continuous.
Care does not end at discharge.
Some bilateral amputees carry higher risk due to age, advanced vascular disease, cardiac weakness, or poor wound history, which can limit safe progression even with strong motivation.
Early identification of these profiles allows clinicians to adjust goals and avoid unsafe expectations.
Risk awareness supports better planning rather than exclusion.
Not all risks are fixed, as weakness, balance deficits, or emotional distress can often improve with targeted intervention.
Clinicians should distinguish between factors that can change and those that cannot.
This distinction helps decide whether to delay, modify, or proceed.
Response to pre-prosthetic training often reveals true potential.
Patients who show steady adaptation and learning tend to progress further.
Early observation is often more reliable than prediction alone.
Bilateral rehabilitation benefits from clear phases that move from sitting balance to standing and then to controlled walking.
Skipping stages increases fall risk and frustration.
Structure builds confidence and safety.
Transfers often matter more than walking distance in daily life.
Learning safe movement between bed, chair, and toilet restores independence early.
These skills reduce caregiver burden.
Bilateral prosthetic walking consumes high energy.
Teaching pacing, rest planning, and efficient movement protects endurance.
Energy management improves long-term use.
Without a natural limb to rely on, balance must be learned consciously.
Patients use visual cues and trunk control to stay upright.
Training should focus on awareness, not speed.
Fear can limit effort and slow learning.
Gradual exposure and controlled environments reduce anxiety.
Confidence grows with safe repetition.
Early training within safe supports allows exploration without danger.
This setting encourages learning without panic.
Removing supports too early increases risk.
Patients must rebuild identity as movers and independent individuals.
This process takes time and emotional support.
Clinicians should expect emotional shifts.
Bilateral patients often compare themselves to unilateral users.
These comparisons can discourage progress.
Reframing success as personal helps.
Motivation may fluctuate during months of training.
Small milestones and recognition support persistence.
Encouragement must be realistic.
Regular use, even for short durations, predicts better long-term outcomes.
Inconsistent use often signals unresolved discomfort or fear.
Monitoring patterns helps early intervention.
Bilateral users place higher stress on hips, back, and shoulders.
Proper alignment and posture protect long-term health.
Regular assessment prevents secondary injury.
Success is defined by safe movement at home and in the community.
Uneven ground and crowds pose challenges.
Gradual exposure improves confidence.
Optimism without evidence can set patients up for disappointment.
Clinicians should base goals on observed performance.
Honesty protects trust.
Rapid escalation increases fatigue and injury risk.
Gradual increase supports tissue tolerance.
Patience prevents setbacks.
Caregivers often experience physical and emotional stress.
Ignoring this strain affects patient outcomes.
Support systems must be assessed.
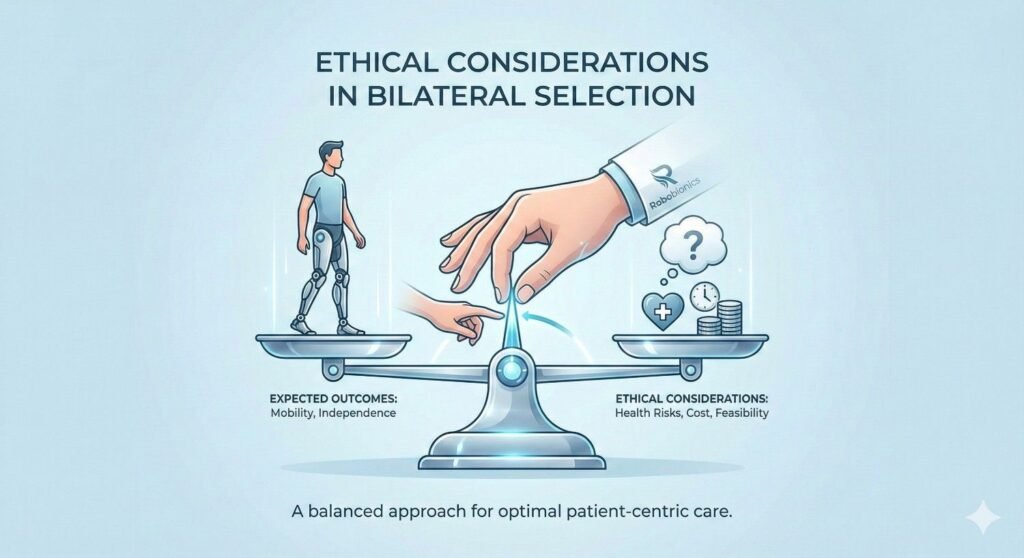
Clinicians must balance the desire to restore walking with realistic risk.
Overpromising harms patients emotionally.
Ethical care values safety.
Some patients value transfers and independence more than walking distance.
These goals are valid.
Respect improves satisfaction.
Bilateral amputation alone should not disqualify patients.
Individual assessment reveals potential.
Fair evaluation preserves dignity.
Clinicians help patients navigate possibility and limitation.
Guidance builds partnership.
This role supports adherence.
Physicians, therapists, prosthetists, and counselors must work together.
Unified goals prevent confusion.
Team care improves outcomes.
Health and capacity change over time.
Regular reassessment allows adaptation.
Care is ongoing.
Bilateral amputees often present with a wider range of medical vulnerabilities than unilateral patients, and some profiles carry a clearly higher risk even when motivation and intent are strong.
Advanced age, severe vascular disease, reduced cardiac reserve, chronic lung disease, or a long history of wound complications can significantly limit safe rehabilitation potential.
Early identification of these profiles allows clinicians to shift focus from ideal outcomes to achievable ones, preventing unsafe expectations while still preserving dignity and purpose.
In bilateral cases, risk factors rarely exist in isolation, and their combined effect can be greater than the sum of individual issues.
For example, moderate heart disease combined with balance deficits and visual impairment may create a higher fall risk than any single condition alone.
Understanding this interaction helps clinicians anticipate challenges before they appear during training.
Recognizing risk does not mean denying prosthetic rehabilitation, but rather shaping it responsibly.
Risk stratification allows clinicians to decide on pacing, support level, device complexity, and outcome goals that protect patient safety.
When risk is acknowledged early, rehabilitation plans become more sustainable and humane.
Not all limiting factors are fixed, as weakness, poor endurance, balance deficits, and even emotional distress often improve with targeted rehabilitation and time.
Patients who initially appear unsuitable may show meaningful gains after structured conditioning or medical optimization.
Clinicians should view early assessments as dynamic rather than final judgments.
Some limitations, such as severe cardiopulmonary disease, progressive neurological conditions, or irreversible joint damage, may cap achievable outcomes despite best efforts.
Identifying these absolute limits helps clinicians avoid unsafe escalation or false reassurance.
Clear recognition protects both patient and care team from prolonged frustration.
Distinguishing between fixed and modifiable risks requires repeated observation rather than a single evaluation.
Short trials of conditioning or balance training often clarify whether improvement is possible.
This approach allows decisions to evolve based on evidence rather than assumption.
Response to pre-prosthetic and early prosthetic training often reveals more about long-term potential than static assessments alone.
Patients who adapt to instructions, improve balance awareness, and tolerate incremental challenges tend to progress further over time.
Early functional response is often the most honest indicator of readiness.
Slow early progress does not always predict failure, especially in older or medically complex patients.
What matters more is consistency, safety awareness, and gradual improvement rather than speed.
Clinicians should look for learning patterns rather than immediate performance.
Judging potential too early may exclude patients who simply need more time or different strategies.
Conversely, ignoring early warning signs of unsafe adaptation may expose patients to injury.
Balanced interpretation of early performance protects long-term outcomes.
Bilateral rehabilitation requires a clearly staged approach that respects the absence of a natural support limb and the higher cognitive and physical demands involved.
Progression should move deliberately from sitting balance and weight shifting to supported standing and finally to controlled stepping.
Skipping phases often leads to fear, falls, and loss of confidence.
Structure reduces uncertainty and anxiety by giving patients clear expectations and achievable milestones.
Knowing what comes next helps patients remain engaged during long rehabilitation timelines.
Predictable progression builds trust in the process.
While progression must be cautious, excessive delay can reduce motivation and conditioning.
Clinicians must strike a balance between protection and forward movement.
Small, regular gains sustain engagement.
For many bilateral amputees, the ability to transfer safely between bed, chair, toilet, and wheelchair defines independence more than walking distance.
These skills reduce reliance on caregivers and restore a sense of control early in rehabilitation.
Clinicians should prioritize transfers as primary goals.
Learning how to move safely on the floor and return to standing after a fall is essential for long-term safety.
Fear of being unable to get up often limits confidence more than fear of walking itself.
Teaching these skills early improves psychological security.
When patients master transfers and basic mobility, caregiver physical and emotional burden decreases significantly.
This reduction improves the overall rehabilitation environment.
Caregiver well-being directly influences patient success.
Walking with two prosthetic limbs requires substantially higher energy expenditure than unilateral walking, especially in older or medically compromised patients.
Fatigue often limits use before mechanical issues appear.
Energy management is therefore a medical necessity, not a comfort measure.
Patients must learn to plan activity with rest periods rather than pushing until exhaustion.
This approach preserves endurance and reduces injury risk.
Clinicians should normalize rest as a strategy, not a failure.
Patients who learn efficient movement patterns and pacing sustain prosthetic use longer.
Energy awareness protects cardiovascular health.
This skill supports lifelong mobility.
Without a biological limb to rely on, bilateral amputees must consciously learn balance strategies using vision, trunk control, and controlled movement.
Balance is no longer automatic and requires attention.
Training should emphasize awareness and control rather than speed or distance.
Fear of falling is common and can severely limit participation if not addressed directly.
Gradual exposure within safe environments allows confidence to grow without overwhelming the patient.
Confidence develops through repeated success, not reassurance alone.
Parallel bars and other support systems provide a controlled space where patients can explore movement safely.
This environment reduces panic and allows focus on technique.
Removing support too early often leads to setbacks.
Bilateral amputation often disrupts how patients see themselves as independent adults, workers, or caregivers.
Rebuilding this identity takes time and emotional support alongside physical training.
Clinicians should expect shifts in mood and self-perception.
Bilateral patients frequently compare themselves to unilateral users, which can create unrealistic expectations or discouragement.
Helping patients focus on personal progress rather than comparison supports emotional stability.
Reframing success as individual reduces frustration.
Motivation naturally fluctuates during extended rehabilitation.
Recognizing effort, celebrating small gains, and setting short-term goals help maintain engagement.
Encouragement must remain realistic to preserve trust.
Regular prosthetic use, even in short sessions, predicts better long-term adaptation and skill retention.
Inconsistent use often signals unresolved discomfort, fear, or poor alignment.
Monitoring use patterns allows early intervention.
Bilateral prosthetic users place increased load on hips, spine, shoulders, and upper limbs.
Poor alignment or posture can lead to chronic pain and secondary disability.
Regular biomechanical review is essential.
True success is measured by safe and confident movement at home and in the community.
Uneven terrain, crowds, and daily unpredictability present challenges that clinic training alone cannot replicate.
Gradual exposure builds competence and confidence.
Optimism unsupported by functional evidence can lead to disappointment and loss of trust.
Clinicians should ground goals in observed ability rather than ideal outcomes.
Honest communication protects morale.
Rapid escalation in wear time increases fatigue, pain, and injury risk.
Gradual progression allows tissues and confidence to adapt.
Patience prevents long-term setbacks.
Caregivers often carry significant physical and emotional responsibility during bilateral rehabilitation.
Unchecked strain can affect patient progress and home safety.
Support systems must be assessed regularly.
Clinicians must balance the desire to restore walking with realistic appraisal of medical and functional risk.
Overpromising can cause emotional harm and unsafe behavior.
Ethical care prioritizes safety alongside hope.
Some patients value independence in transfers and self-care more than walking distance or appearance.
These priorities are valid and should guide rehabilitation goals.
Respect improves satisfaction and adherence.
Bilateral amputation alone should never automatically disqualify a patient from prosthetic consideration.
Individual assessment often reveals unexpected potential.
Fair evaluation preserves dignity.

Clinicians are not merely deciding access to prosthetics, but guiding patients through realistic possibilities and limitations.
This partnership approach builds trust and long-term engagement.
Guidance supports adherence.
Successful bilateral rehabilitation requires coordination between physicians, therapists, prosthetists, and mental health professionals.
Unified goals prevent mixed messages and confusion.
Team care strengthens outcomes.
Health, strength, and priorities change over time, especially in chronic disease.
Regular reassessment allows adaptation of prosthetic goals and strategies.
Bilateral prosthetic care is a long-term journey, not a single decision.
At Robobionics, we have learned that bilateral prosthetic rehabilitation is never a single decision or a short phase of care, but a long-term partnership between clinicians, patients, families, and the prosthetic team.
Outcomes are shaped not only by devices, but by timing, selection, expectation setting, and continuous guidance as the patient’s body and confidence change.
When clinicians approach bilateral cases with patience and structure, results become more predictable and humane.
Careful selection is not meant to deny opportunity, but to protect patients from unsafe paths and emotional harm caused by unrealistic goals.
Clear criteria help clinicians decide when to proceed, when to slow down, and when to redefine success.
This clarity builds trust and prevents avoidable failure.
Success for bilateral amputees often looks different from textbook walking outcomes and must be measured through independence, safety, and quality of life.
Transfers, short-distance walking, self-care, and confidence in daily routines matter deeply to patients.
Clinicians who redefine success help patients stay engaged and satisfied.
Bilateral rehabilitation rewards gradual, well-paced progression far more than aggressive timelines.
Early patience preserves energy, prevents injury, and supports long-term use.
Timing remains one of the most powerful clinical tools available.
As an Indian prosthetics manufacturer, Robobionics works closely with clinicians managing complex bilateral cases across varied medical and social settings.
Our focus is on affordable, lightweight, and serviceable prosthetic solutions that support staged rehabilitation and real-world use.
By aligning thoughtful selection with adaptable prosthetic design, we aim to help clinicians restore mobility, dignity, and realistic independence for bilateral amputees across India.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body