
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


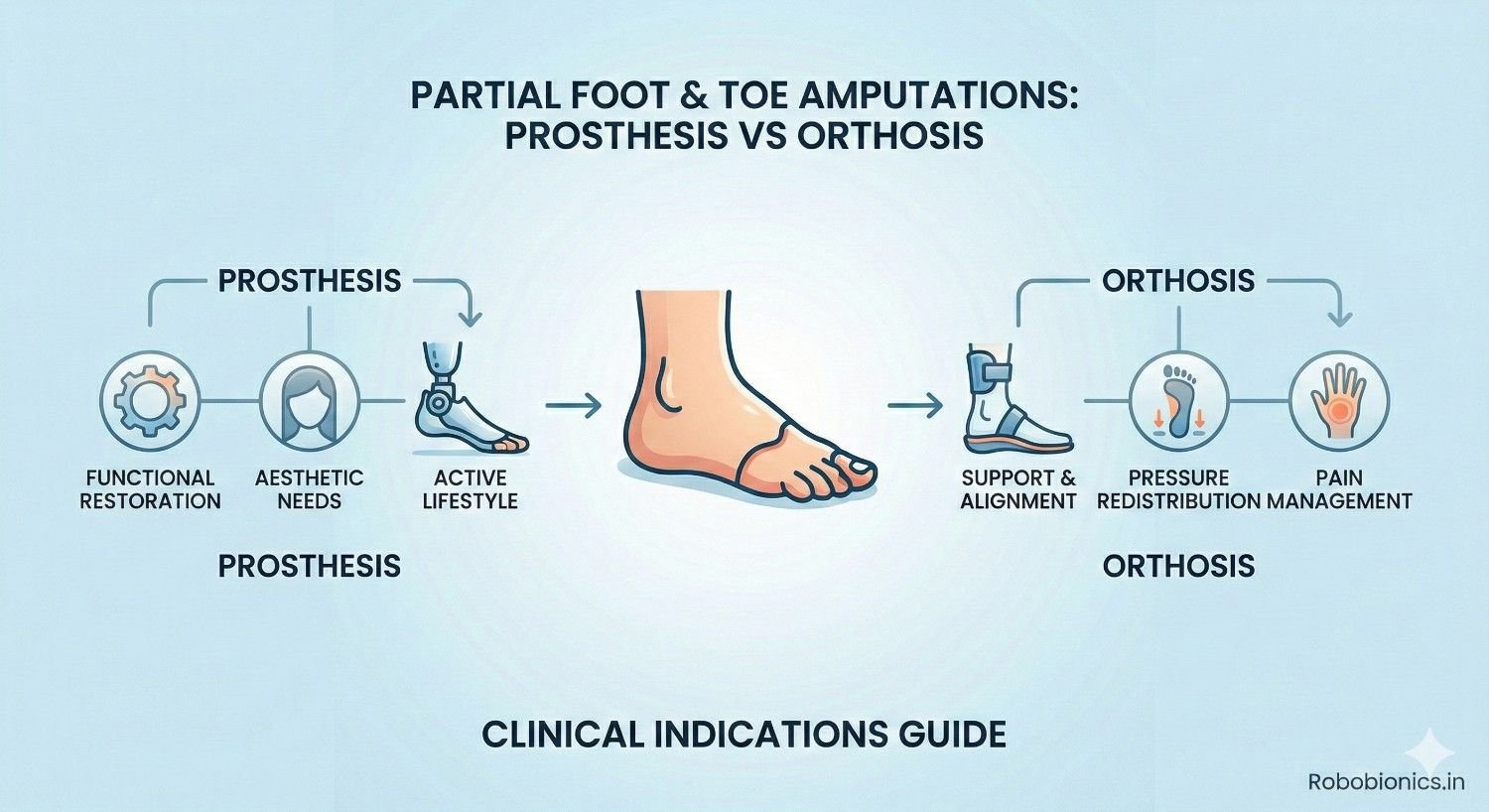
Partial foot and toe amputations are often seen as minor compared to higher-level limb loss, but their impact on walking, balance, and long-term foot health can be significant. Losing even a small part of the foot changes how weight is transferred, how muscles work, and how stable each step feels. This is why deciding between a prosthesis and an orthosis after partial foot or toe amputation is never a simple choice.
At Robobionics, we frequently meet patients who are told they may not need any device at all, only to develop pain, skin breakdown, or walking problems months later. We also see patients placed into prostheses that are heavier or more complex than needed, which reduces comfort and daily use. The real challenge lies in understanding when a prosthesis is truly required and when a well-designed orthosis can offer better function and protection.
This article focuses on partial foot and toe amputations and explains the clinical indications for choosing a prosthesis versus an orthosis. It looks closely at how different amputation levels affect gait, how load is redistributed across the foot, and how device choice influences long-term outcomes. The goal is clarity, not complexity.
If you are a doctor, therapist, or patient navigating this decision, this guide will help you understand the functional differences and make choices that support comfort, safety, and durability. The right solution is not about replacing what is lost, but about restoring stable and confident movement.
Even a small loss in the foot changes how the body moves.
The toes and forefoot play a major role in balance, push-off, and shock absorption during walking.
When part of the foot is missing, the body must quickly adapt to a new load pattern.
Patients often feel unstable without clearly understanding why.
This instability may not appear immediately but develops over weeks or months.
Early understanding helps prevent long-term problems.
Most partial foot and toe amputations happen due to diabetes, infection, or poor blood flow.
Trauma and tumors are less common but still important causes.
The underlying cause strongly affects healing and device choice.
Patients with diabetes often have nerve loss and poor circulation.
This increases the risk of skin breakdown after amputation.
Device decisions must protect the remaining foot carefully.
Leaving a partial foot amputation unsupported can cause secondary damage.
Excess pressure shifts to areas not designed to carry it.
This leads to ulcers, joint pain, and altered walking patterns.
Early intervention with the right device prevents these issues.
Waiting until pain develops often makes correction harder.
Proactive planning protects long-term mobility.
Toes help stabilize the body during standing and slow walking.
They widen the base of support and provide sensory feedback.
Loss of toes reduces this natural balance system.
Patients may feel fine on flat ground but struggle on uneven surfaces.
Turning and stopping become less controlled.
These issues increase fall risk over time.
The forefoot is critical during the push-off phase of walking.
It stores and releases energy with each step.
Loss of forefoot length reduces walking efficiency.
Patients often compensate by overusing the ankle or knee.
This increases fatigue and joint strain.
Over time, pain may develop in other areas.
Partial foot loss often leads to uneven walking patterns.
Stride length and timing change unconsciously.
The body favors the intact side.
Gait asymmetry increases stress on hips and lower back.
These changes may not cause pain immediately.
Long-term effects can be significant.
Single or multiple toe amputations seem minor but still affect balance.
Loss of the big toe has the greatest impact.
It alters push-off and stability significantly.
Smaller toe losses may cause subtle changes.
These changes accumulate over time.
Proper support helps reduce compensation.
Toe amputations often do well with orthotic solutions.
Prostheses are rarely required at this level.
However, assessment must be individualized.
Ray amputations remove a toe and part of the metatarsal.
This shortens the forefoot and shifts weight laterally or medially.
Balance becomes more difficult.
Patients often develop calluses or ulcers at new pressure points.
Footwear alone is usually insufficient.
Support must control load distribution.
At this level, advanced orthoses or prosthetic fillers may be needed.
The decision depends on stability and skin tolerance.
Functional testing guides choice.
Transmetatarsal amputations remove a large part of the forefoot.
Push-off is severely reduced.
Walking becomes less efficient.
Midfoot amputations further shorten lever arm length.
The ankle must work harder to compensate.
Energy cost rises noticeably.
These levels often require prosthetic solutions.
Orthoses alone may not provide enough leverage.
Stability and protection become priorities.
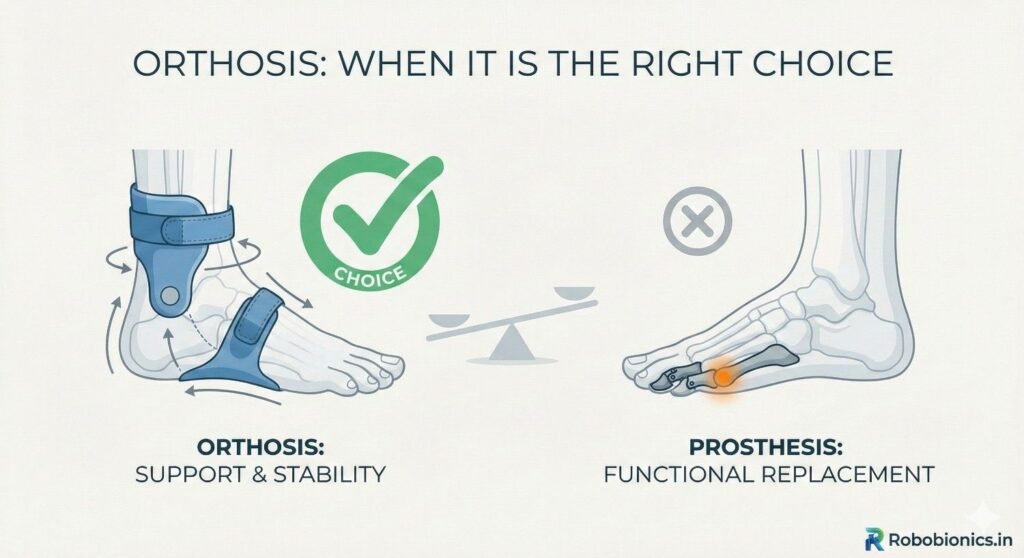
An orthosis supports and protects the remaining foot.
It redistributes pressure and improves alignment.
It works within the shoe.
Orthoses preserve natural foot movement as much as possible.
They are lighter and easier to manage.
This makes them attractive for early intervention.
Orthoses aim to prevent further damage.
They are protective rather than replacing missing anatomy.
Their role is often underestimated.
Orthoses work well when enough foot length remains.
Patients must have reasonable balance and strength.
Skin condition must tolerate shoe-based support.
Toe and partial ray amputations often respond well.
Early forefoot loss may still benefit from orthoses.
Comfort and stability guide this choice.
Patients with good ankle control usually do better.
Orthoses rely on existing joints.
Functional testing confirms suitability.
Orthoses are easier to wear and maintain.
They fit into standard footwear.
This improves daily compliance.
They allow more natural walking patterns.
Patients often feel less restricted.
Adaptation is quicker.
Orthoses also allow easy adjustments.
Changes in foot shape can be accommodated.
This flexibility is valuable in diabetic patients.
Orthoses cannot replace lost push-off power.
When forefoot length is too short, leverage is insufficient.
Walking remains inefficient.
Patients may still feel unstable despite good orthotic design.
Fatigue appears quickly.
Compensation increases.
At this point, orthoses may delay necessary prosthetic intervention.
Recognizing failure early is important.
Escalation improves outcomes.
Poorly designed orthoses can create pressure points.
This is dangerous in patients with reduced sensation.
Ulcers may develop unnoticed.
Frequent review is essential.
Skin must be monitored closely.
Early signs require immediate adjustment.
Orthoses are only safe when properly fitted.
Generic solutions often fail.
Customization is critical.
As amputation level moves proximally, orthoses lose effectiveness.
They cannot restore lever length.
They only cushion what remains.
At transmetatarsal and midfoot levels, this becomes clear.
Patients struggle with stairs and uneven ground.
Prosthetic solutions often work better.
Doctors must recognize this threshold.
Delaying prosthetic fitting increases strain.
Timely transition improves function.
A partial foot prosthesis replaces lost length and shape.
It restores a lever for push-off.
This improves walking efficiency.
The prosthesis works as an extension of the foot.
It often includes a filler and support shell.
This stabilizes the ankle and foot.
Prostheses shift load away from vulnerable areas.
They protect the remaining foot.
This is crucial in high-risk patients.
Prostheses are indicated when forefoot loss is significant.
Instability during walking is a key sign.
Failure of orthotic management also guides this decision.
Patients with transmetatarsal or midfoot amputations often need prostheses.
Energy loss becomes too great otherwise.
Balance improves with added structure.
Skin health also influences the choice.
Prostheses can offload pressure effectively.
This reduces ulcer risk.
Prosthetic users often walk more symmetrically.
Stride length improves.
Fatigue decreases.
Stability increases during standing and turning.
Confidence improves noticeably.
This encourages activity.
Prostheses also support long-term joint health.
They reduce compensatory stress.
This protects knees, hips, and back.
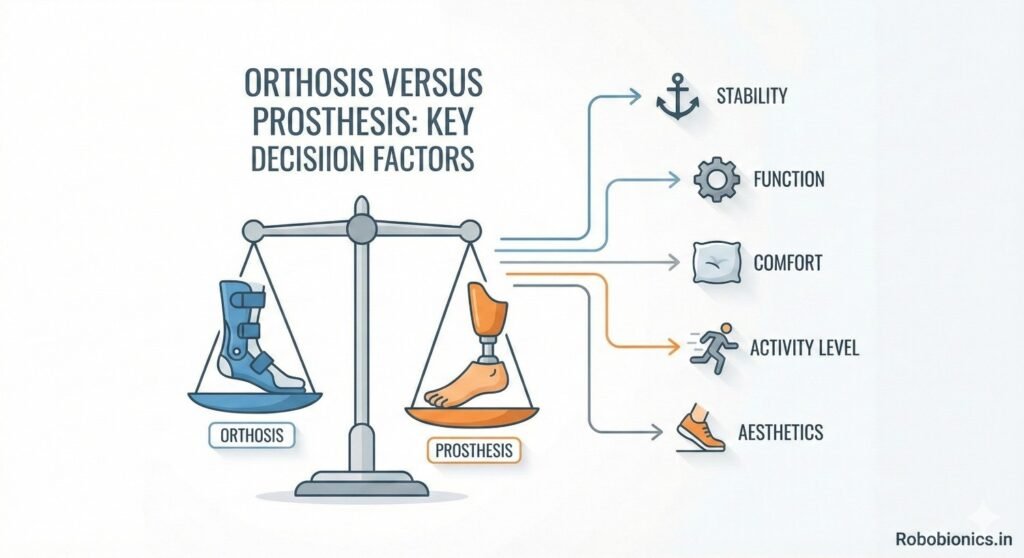
Foot length is one of the strongest indicators.
More remaining length favors orthoses.
Less length favors prostheses.
Doctors should assess effective lever arm, not just appearance.
Functional testing clarifies this.
Visual assessment alone is misleading.
This factor must be considered early.
Delays increase compensations.
Timely decisions improve adaptation.
Patients with reduced sensation need careful load control.
Orthoses may create hidden pressure points.
Prostheses may distribute load more evenly.
Tissue quality affects tolerance.
Fragile skin requires protective solutions.
Device choice must prioritize safety.
Regular skin inspection is essential.
Education supports early detection.
Prevention is better than treatment.
Active patients with good balance may manage with orthoses longer.
Lower activity patients may benefit from prostheses earlier.
Endurance matters.
Balance deficits favor prosthetic stability.
Orthoses rely on neuromuscular control.
Assessment must be honest.
Activity goals guide decisions.
Daily walking demands should be realistic.
Device choice must match lifestyle.
Watching how a patient walks without support provides valuable information.
Subtle limping, shortened steps, or early heel rise often indicate loss of forefoot leverage.
These signs may appear even when the patient reports feeling fine.
Doctors should observe walking on flat ground and during turns.
Difficulty controlling speed or stopping smoothly is important.
These findings often predict long-term issues.
Barefoot observation should be brief and safe.
It is not for endurance testing.
It simply reveals natural compensation patterns.
Temporary fillers or trial orthoses can clarify needs.
Improved stability with support suggests benefit from a device.
Lack of improvement signals need for a different approach.
Patients often feel the difference immediately.
This feedback is valuable.
It helps guide shared decisions.
Short trials reduce guesswork.
They allow real-world observation.
Clinical confidence improves.
Partial foot loss increases energy cost during walking.
This may not be obvious in short distances.
Longer observation reveals fatigue patterns.
Patients may slow down or rely more on the intact side.
These changes stress other joints.
Early detection prevents secondary pain.
Energy efficiency is a key goal.
Devices should reduce effort, not add to it.
Gait analysis supports this aim.
Unprotected partial foot amputations often develop ulcers.
Pressure shifts to areas not designed to bear weight.
This is common in diabetic patients.
Ulcers may start small and painless.
They worsen quickly if unnoticed.
Delayed intervention increases infection risk.
Proper device choice reduces pressure peaks.
Both orthoses and prostheses can help when chosen correctly.
Prevention is always preferable.
Compensatory walking patterns strain joints over time.
Knees, hips, and the lower back are most affected.
Pain often appears months after amputation.
Patients may not connect joint pain to foot loss.
This delays appropriate treatment.
Early support prevents this cascade.
Reducing asymmetry protects the entire body.
Device choice has long-term implications.
Whole-body health must be considered.
Instability and fatigue reduce confidence.
Patients begin limiting activity to avoid discomfort.
This leads to deconditioning.
Reduced activity worsens balance and strength.
The problem compounds itself.
Timely support breaks this cycle.
Devices should encourage movement, not restrict it.
Comfort and stability restore confidence.
This supports independence.
Many diabetic patients have reduced foot sensation.
They may not feel pressure or injury.
This increases risk with poorly fitted devices.
Orthoses must be carefully designed and monitored.
Prostheses may offer better load distribution.
Frequent follow-up is essential.
Education on daily skin checks is critical.
Patients must understand warning signs.
Support systems matter.
Poor blood flow affects healing and tolerance.
Skin may break down easily.
Device-induced pressure must be minimized.
Doctors should assess vascular status before deciding.
Healing capacity guides aggressiveness of intervention.
Safety must guide choice.
Sometimes simpler solutions are safer initially.
Progression may be gradual.
Flexibility improves outcomes.
Inadequate support increases risk of further tissue loss.
Repeated ulcers may lead to higher-level amputation.
This is a serious consequence.
Choosing the right device early reduces this risk.
Protecting remaining tissue is paramount.
Long-term thinking is essential.
Footwear plays a major role in device success.
Orthoses rely on proper shoes for effectiveness.
Poor footwear limits benefit.
Prostheses may require custom shoes or inserts.
Patients must be willing to adapt.
Lifestyle compatibility matters.
Doctors should discuss footwear early.
Surprises reduce compliance.
Preparation improves acceptance.
Patients who stand or walk for long periods need durable solutions.
Orthoses may fatigue faster under heavy use.
Prostheses often provide better endurance.
Work surfaces also matter.
Uneven ground increases instability.
Device choice must reflect environment.
Activity goals should be realistic.
Overambition leads to disappointment.
Honest planning supports success.
Some patients worry about appearance.
Bulky devices may cause resistance.
This affects daily use.
Doctors should acknowledge these concerns.
Education and design options help.
Acceptance improves with understanding.
Comfort and function usually outweigh cosmetic issues over time.
Early reassurance helps patients adapt.
Respectful discussion matters.
Orthotic solutions may work initially but fail over time.
Increasing fatigue, pain, or instability are warning signs.
These should prompt reassessment.
Doctors should not view transition as failure.
It reflects changing needs.
Adaptation is part of care.
Early recognition prevents prolonged discomfort.
Patients progress faster with the right support.
Timely transition improves outcomes.
Patients may resist moving to a prosthesis.
Fear of complexity or stigma is common.
Education reduces anxiety.
Explaining functional benefits helps.
Demonstrations can be effective.
Seeing improvement builds confidence.
Gradual transition plans work best.
Patients feel supported.
Trust is preserved.
Before transitioning, reassessment is essential.
Strength, balance, and skin health should be reviewed.
Goals may need adjustment.
Prosthetic trials can clarify benefit.
Temporary fittings provide insight.
Patient feedback is valuable.
Reassessment ensures readiness.
Safety remains the priority.
Structured planning supports success.
Choosing between prosthesis and orthosis requires teamwork.
Doctors, prosthetists, and therapists each bring expertise.
Collaboration improves decisions.
Shared assessment reduces bias.
Different perspectives highlight different risks.
Unified plans support patients better.
Patients benefit from coordinated messaging.
Conflicting advice undermines trust.
Team alignment is essential.
Generic solutions rarely work well.
Partial foot loss varies widely.
Customization improves comfort and function.
Both orthoses and prostheses require precise design.
Small adjustments make big differences.
Attention to detail matters.
Ongoing refinement is normal.
Devices evolve with patient needs.
Flexibility supports long-term use.
Patients need education on use and care.
Daily inspection and maintenance are critical.
Neglect leads to complications.
Regular follow-up detects issues early.
Adjustments prevent breakdown.
Long-term success depends on monitoring.
Providers must emphasize this commitment.
Care does not end at fitting.
Support is ongoing.
Proper device choice improves mobility significantly.
Patients walk more confidently and efficiently.
Independence increases.
Confidence encourages activity.
Activity supports overall health.
This creates positive momentum.
Poor choices limit potential.
Patients may withdraw.
Correct decisions unlock capability.
Supporting the foot properly protects the whole body.
Joint pain and back issues are reduced.
Energy efficiency improves.
Preventing ulcers avoids hospitalizations.
Quality of life improves.
Healthcare costs decrease.
Early investment in the right device pays off.
Long-term benefits are substantial.
Prevention is powerful.
Feeling stable restores confidence.
Patients worry less about falling.
Mental stress decreases.
Independence supports self-esteem.
Patients feel more in control.
This improves overall outlook.
Device choice affects more than movement.
It affects identity and confidence.
Holistic care matters.
Partial foot and toe amputations require careful attention, even when they appear minor.
The decision between a prosthesis and an orthosis must be based on function, not assumptions or convenience.
Foot length, stability, skin health, and activity demands all play crucial roles.
At Robobionics, our experience shows that early, thoughtful intervention prevents many long-term problems.
Neither prostheses nor orthoses are universally better.
The right choice depends on the individual and may change over time.
When clinicians and patients work together to evaluate real-world function, outcomes improve.
Comfort, safety, and confidence become achievable goals.
The best solution is the one that supports stable, pain-free movement for the long term.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body