
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Upper-limb loss affects how a person works, communicates, and connects with the world, often more visibly than many other physical injuries. Myoelectric prosthetics offer powerful functional benefits, but they are not right for every patient or at every stage of recovery. For doctors, selecting the ideal candidate requires more than checking muscle signals; it demands a clear understanding of learning ability, motivation, daily needs, and long-term commitment.
This article explains the ideal patient profiles for upper-limb myoelectric prosthetics in a clear and practical way for MDs. It focuses on medical readiness, muscle control, cognitive ability, emotional preparedness, and real-life use, helping clinicians decide who will benefit most and how to guide patients toward successful adoption.
Myoelectric prosthetics use natural muscle signals from the residual limb to open, close, or move the hand, which allows users to control the device by thinking about movement rather than using body-powered force.
These signals must be strong, repeatable, and well isolated for reliable control.
Understanding this basic principle helps doctors predict who will adapt well.
Unlike passive or body-powered hands, myoelectric devices require the user to learn signal control, timing, and coordination through practice.
The device responds only as well as the user can train their muscles and attention.
This learning demand makes patient selection critical.
Myoelectric hands are most useful when patients need precise grip, better appearance, or reduced physical strain.
They may be unnecessary for patients with very limited functional demands.
Selection should always begin with real-life use cases.
Below-elbow amputations usually offer the best outcomes with myoelectric hands due to preserved forearm muscles.
These muscles produce clearer signals and allow finer control.
Transradial patients often adapt faster and with less fatigue.
Above-elbow or shoulder-level amputations can still use myoelectric systems, but control becomes more complex.
Fewer available muscle sites and higher cognitive load slow learning.
Expectations must be adjusted carefully.
Adequate residual limb length improves socket fit and signal consistency.
Very short stumps may struggle with electrode placement.
Socket stability directly affects control reliability.
Ideal candidates can activate specific muscle groups without unwanted co-contraction.
Clear separation between signals allows smoother control.
Poor isolation increases frustration.
Severe scarring or muscle loss can reduce signal strength.
These factors do not always exclude use, but they increase training needs.
Assessment should include dynamic testing, not just rest exams.
Myoelectric control can degrade with fatigue.
Patients with low endurance may struggle with long use sessions.
Fatigue tolerance should be considered early.
While myoelectric hands do not restore natural sensation, users rely on visual and pressure cues.
Patients must tolerate this indirect feedback style.
Those expecting natural feeling may be disappointed.
Persistent pain or severe sensitivity reduces tolerance to socket wear.
Pain also interferes with muscle control learning.
Pain management should come before fitting.
Healthy skin ensures consistent electrode contact.
Frequent sweating, breakdown, or infection disrupts control.
Skin readiness is part of candidacy.
Users must understand how muscle activation leads to prosthetic movement.
This cognitive link is essential for progress.
Patients who grasp this concept early tend to succeed.
Myoelectric training requires focused practice.
Distractibility slows learning and increases errors.
Doctors should assess attention capacity.
Many myoelectric systems involve grip selection or mode switching.
Remembering sequences is necessary for functional use.
Cognitive screening helps set realistic expectations.
Daily practice is essential for mastering control.
Patients unwilling or unable to practice regularly struggle.
Motivation must be intrinsic.
Initial control often feels unnatural and slow.
Patients who tolerate frustration adapt better.
Low frustration tolerance predicts abandonment.
Comfort with technology affects learning speed.
Patients open to devices and feedback adapt faster.
Fear of technology may require extra support.
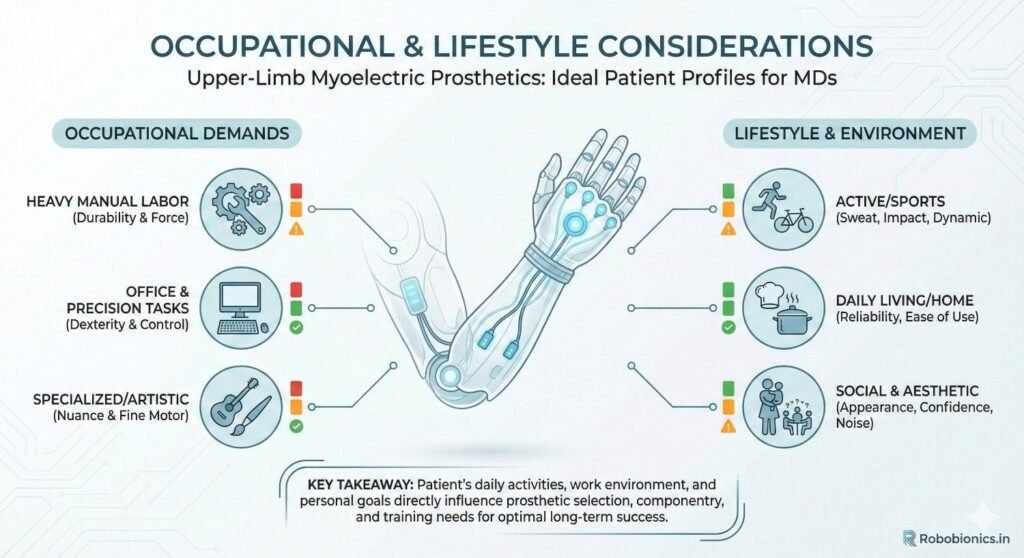
Jobs requiring fine motor control or frequent hand use benefit most from myoelectric hands.
Manual laborers may prefer durable alternatives.
Work context shapes device choice.
Tasks like eating, grooming, and social gestures are often easier with myoelectric hands.
Appearance can influence social confidence.
Lifestyle goals should guide selection.
Myoelectric devices need charging and basic care.
Patients must manage these tasks reliably.
Maintenance ability affects long-term success.
Children and teens can adapt well if cognitive readiness is present.
Growth requires frequent adjustments.
Family support becomes critical.
Age alone does not exclude candidacy, but learning pace may be slower.
Patience and support matter more than age.
Doctors should focus on adaptability, not years.
Early fitting can support brain adaptation, but readiness matters more than speed.
Delayed fitting remains effective when motivation is strong.
Timing should be individualized.
Supportive families reinforce practice and care routines.
Overpressure can cause resistance.
Balanced support improves outcomes.
Regular therapy sessions improve skill acquisition.
Limited access may slow progress.
This factor should be discussed openly.
Seeing others use myoelectric hands builds confidence.
Peer interaction reduces fear.
Doctors can facilitate these connections.
Myoelectric hands restore function, not natural sensation.
Clear explanation prevents disappointment.
Expectation setting is clinical care.
Skill develops over months, not days.
Early progress may be subtle.
Patience is essential.
Success varies by individual goals.
Partial use can still be meaningful.
Clinicians should personalize outcomes.
Successful myoelectric use often begins even before the prosthesis is fitted, because patients must learn how to activate and relax specific muscles in a controlled way.
Early muscle training builds awareness and confidence, which reduces frustration once the device is introduced.
Doctors who encourage pre-fitting training often see smoother transitions.
Once the device is fitted, learning must follow a structured path that starts with simple open and close actions before moving to more complex grips.
Skipping basic control stages usually leads to confusion and poor long-term skill.
Structure provides predictability and safety during learning.
Occupational therapy helps patients translate muscle control into real-life tasks such as eating, dressing, and object handling.
These daily wins build confidence faster than abstract exercises.
Functional success reinforces motivation.
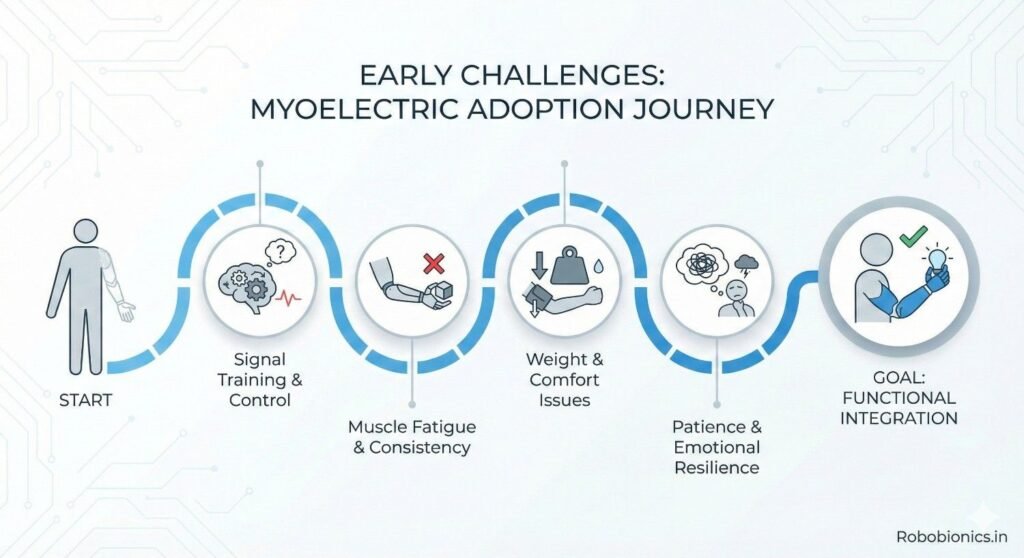
Many patients feel disappointed during early sessions because movements feel slow or inaccurate.
This phase is normal and temporary but must be explained clearly.
Doctors should normalize this experience to prevent early dropout.
Learning myoelectric control is mentally demanding, especially in the first weeks.
Patients may tire cognitively before they tire physically.
Shorter, focused sessions work better than long ones.
Some patients expect instant smooth movement based on videos or demonstrations.
When reality differs, disappointment can arise.
Revisiting expectations protects morale.
Inconsistent signals lead to unpredictable movement, which frustrates users.
This issue may arise from poor socket fit, fatigue, or muscle imbalance.
Technical review should always come before judging patient failure.
Some patients use the device less after the first few weeks.
This pattern often signals discomfort, fear, or unmet expectations.
Early follow-up helps identify the cause.
If the prosthesis remains a clinic-only device, long-term use is unlikely.
Integration into daily routines is essential.
Doctors should ask how often and where the device is used.
Patients who practice regularly, even briefly each day, develop smoother control over time.
Consistency matters more than session length.
Habit predicts mastery.
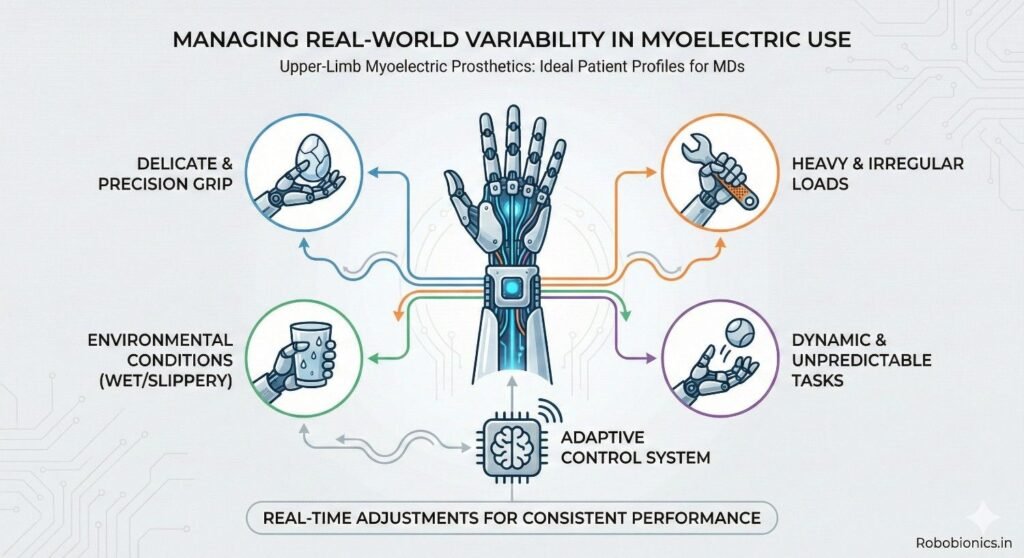
Myoelectric users must adjust grip and force across tasks.
Those who enjoy problem-solving adapt better.
Flexibility supports long-term success.
Charging, cleaning, and basic care are part of ownership.
Patients who manage maintenance confidently experience fewer interruptions.
Practical ability supports adherence.
Some patients prefer body-powered hands due to simplicity and durability.
These devices may suit heavy labor or limited training access.
Choice should respect lifestyle needs.
Some users start with simpler devices and transition to myoelectric later.
This staged approach reduces overwhelm.
Progression can be planned.
The most advanced option is not always the best option.
Patient fit matters more than features.
Clinicians should guide, not sell.
Advanced technology can create unrealistic hope.
Doctors must ground recommendations in patient capability.
Honesty protects trust.
Some patients may decline myoelectric options after understanding demands.
This choice should be respected.
Autonomy is part of care.
Cost, service access, and durability affect long-term success.
Sustainable solutions matter more than novelty.
Clinicians should consider the full journey.
Control improves gradually with practice.
Follow-up allows adjustment of training goals.
Progress should be reviewed regularly.
New jobs, health changes, or family needs can alter device use.
Reassessment ensures continued relevance.
Flexibility supports longevity.
Early identification of frustration prevents abandonment.
Support and adjustment keep patients engaged.
Follow-up is preventive care.
Patients should expect gradual improvement rather than sudden transformation.
This mindset reduces disappointment.
Time is a teacher.
Experimenting with grips and tasks builds skill.
Fear of mistakes limits learning.
Safe exploration supports confidence.
Patients should see the prosthesis as a tool, not a definition of self.
This perspective reduces emotional pressure.
Healthy identity supports resilience.
Many patients demonstrate good control during supervised clinic sessions, yet struggle to reproduce the same performance at home where distractions, fatigue, and uneven routines interfere.
This difference does not indicate failure, but rather highlights the need to assess readiness beyond controlled environments.
Doctors should ask patients how the prosthesis feels during real daily tasks, not only how it performs during therapy.
Heat, sweat, dust, and humidity can affect electrode contact and signal quality, especially in Indian conditions.
Patients who can problem-solve around these challenges tend to maintain use more consistently.
Screening should include discussion of the patient’s living and working environment.
A patient who succeeds with a myoelectric hand often learns when to rely on it and when to rest or switch strategies.
This adaptability supports long-term success more than rigid full-time use.
Doctors should frame flexibility as strength, not inconsistency.
Myoelectric prosthesis abandonment rarely happens suddenly and is usually preceded by reduced daily use, frustration, or quiet disengagement.
These signs often appear weeks or months before complete non-use.
Early identification allows corrective action.
Patients who stop practicing, avoid follow-up visits, or describe the device as “too much effort” may be struggling emotionally or technically.
These signals should prompt review of fit, expectations, and support rather than assumptions about motivation.
Timely intervention often restores engagement.
Small changes in socket comfort, training pace, or daily goals can significantly improve adherence.
Doctors who encourage open discussion about difficulty reduce shame and withdrawal.
Proactive support protects long-term outcomes.
Patients often begin with optimistic expectations that naturally shift once daily challenges emerge.
This evolution is healthy when guided, but damaging when ignored.
Clinicians should revisit expectations at multiple stages, not only before fitting.
When patients realize that the prosthesis will not fully replace a biological hand, disappointment may surface.
Acknowledging this honestly while highlighting functional gains helps patients recalibrate goals.
Balanced reassurance supports continued use.
Small achievements such as holding cutlery, managing a phone, or performing work-related tasks often matter more than cosmetic outcomes.
Doctors should reinforce these functional wins consistently.
Recognition builds confidence and persistence.
Myoelectric prosthetics require not only initial investment but also long-term maintenance, servicing, and charging habits.
Patients who understand and plan for these realities cope better over time.
Financial stress can indirectly affect adherence.
Patients living far from service centers or with limited follow-up access may struggle if frequent adjustments are needed.
This does not exclude candidacy, but requires realistic planning and device choice.
Clinicians should factor service pathways into recommendations.
A simpler, well-supported myoelectric solution often outperforms a complex system that cannot be maintained.
Doctors should prioritize durability and serviceability over feature count.
Long-term sustainability defines success.
Patients benefit when doctors present myoelectric use as a learnable skill rather than an automatic solution.
This framing encourages patience and effort.
Skill-based framing reduces unrealistic expectations.
Patients who believe struggle is abnormal tend to disengage quickly.
Doctors who normalize difficulty as part of learning protect motivation.
Language choice matters.
When patients understand their active role in training, care, and feedback, outcomes improve.
Shared responsibility builds ownership.
Ownership sustains use.
Confidence, willingness to try new tasks, and reduced avoidance often signal success earlier than technical metrics.
Doctors should monitor emotional adaptation alongside control quality.
Psychological comfort predicts durability.
Returning to work, social interaction, or hobbies indicates meaningful prosthetic integration.
These markers often matter more to patients than grip strength.
Clinicians should ask about life participation regularly.
Life circumstances change, and prosthetic goals must evolve accordingly.
Reassessment ensures continued relevance of the device.
Adaptation sustains long-term value.
Despite best screening, some patients discover that myoelectric use does not suit their preferences or lifestyle.
Recognizing this early prevents prolonged frustration.
Changing direction is responsible care.
Choosing a different prosthetic option should never be framed as failure.
Respectful redirection preserves dignity and trust.
Clinicians should emphasize fit, not hierarchy.
Some patients may revisit myoelectric options later as circumstances change.
Leaving the option open maintains hope without pressure.
Timing matters.
At Robobionics, we have seen that upper-limb myoelectric prosthetics deliver their best outcomes when technology is matched thoughtfully to the person, not simply to the amputation level.
Patients who succeed are not defined by strength alone, but by learning ability, patience, daily needs, and emotional readiness.
Careful selection protects patients from frustration and protects clinicians from avoidable failure.
Advanced features and multiple grips mean little if the patient cannot train, adapt, and integrate the device into daily life.
When doctors screen muscle control, cognition, motivation, and lifestyle together, myoelectric prosthetics become tools for independence rather than unused equipment.
This screening is not restrictive; it is responsible care.
Myoelectric hands reward consistency, curiosity, and gradual progress, which makes early expectation setting a powerful clinical tool.
Patients who understand that mastery takes time approach rehabilitation with patience and resilience.
Clear conversations early often decide whether the device becomes part of life or stays in a drawer.
Successful myoelectric adoption depends on close collaboration between doctors, therapists, prosthetists, and families.
Each team member sees different aspects of readiness and progress.
Shared insight leads to better timing, better training, and better outcomes.
As an Indian prosthetics manufacturer, Robobionics designs myoelectric solutions like Grippy™ with a strong focus on usability, reliability, and real-world Indian conditions.
We work closely with clinicians to support patient selection, staged training, and long-term follow-up so that technology remains accessible and meaningful.
By combining thoughtful patient profiling with affordable innovation, we aim to help doctors restore function, confidence, and dignity through upper-limb myoelectric prosthetics.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body