
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


A prosthesis can restore function, balance, and confidence when prescribed at the right time for the right person. But there are moments in clinical care when prescribing a prosthesis can do more harm than good. Knowing when not to prescribe is just as important as knowing when to prescribe. This article explains the clinical situations doctors should recognise, where waiting, rethinking, or choosing a different path leads to better outcomes for the patient.
A prosthesis is meant to solve a functional problem in daily life. It is not meant to only look complete or reassure others.
When the problem it is meant to solve is not clearly defined, the device often goes unused.
Doctors must first ask what function is missing and whether a prosthesis can truly help.
In some settings, prostheses are prescribed simply because they are available.
This approach ignores readiness, healing stage, and real need.
Default prescriptions often result in discomfort, frustration, and abandonment.
Saying no does not mean denying care.
It means protecting the patient from an intervention that may harm recovery.
Good clinical judgement includes restraint.
In the early phase after injury or surgery, tissues are often swollen and fragile.
Joints may not be aligned and pain levels may change daily.
Prescribing a prosthesis at this stage can increase stress on healing structures.
Early on, the body often uses protective and awkward movements.
A prosthesis introduced too soon may lock these patterns in place.
These habits are hard to undo later.
In early healing, simple supports or positioning aids may be enough.
These protect alignment without forcing function.
Doctors should avoid jumping to definitive prosthetic solutions too early.
Learning to use a prosthesis requires focus and repetition.
When pain is severe or unpredictable, learning becomes difficult.
Prescribing during this phase often leads to rejection.
Some patients experience extreme skin sensitivity after injury or surgery.
Even light touch can feel unbearable.
A prosthesis can worsen this and increase distress.
Pain control should come first.
Once pain is stable and predictable, prosthetic discussions become more meaningful.
Timing here protects long-term acceptance.
A prosthesis relies on stable joints for control and comfort.
If the shoulder, hip, or spine is unstable, forces are poorly distributed.
This can increase pain and damage.
Early after surgery or trauma, alignment often shifts.
Prescribing before alignment settles leads to repeated refitting.
This frustrates patients and increases cost.
Doctors should focus on stabilising the body first.
A strong base allows the prosthesis to work as intended.
Skipping this step leads to failure.
Using a prosthesis requires understanding safety, limits, and care.
Patients who cannot follow instructions are at risk of injury.
Prescribing in this scenario is unsafe.
Some conditions affect memory or attention span.
This can lead to misuse or neglect of the device.
Doctors must assess cognitive readiness carefully.
If training cannot be absorbed, the device will not be used well.
Waiting or choosing simpler options is often safer.

Acceptance is a process, not a moment.
Some patients are still in shock or denial.
Introducing a prosthesis too early can feel overwhelming.
Depression reduces engagement and effort.
A prosthesis requires active participation to succeed.
Prescribing during severe depression often leads to abandonment.
Emotional support and counselling may be needed before devices.
Mental readiness protects long-term outcomes.
Some patients believe a prosthesis will work like a natural limb.
When reality does not match this belief, disappointment follows.
Doctors should not prescribe until expectations are realistic.
Online videos often show best-case outcomes.
Patients may expect similar results without context.
Education must come before prescription.
Clear goal setting prevents misuse and frustration.
Without this, prescribing does more harm than good.
A prosthesis requires contact and pressure.
Open wounds or fragile skin cannot tolerate this.
Prescribing too early risks infection and breakdown.
Some skin conditions worsen with prosthetic use.
This can cause discomfort and hygiene issues.
Doctors should stabilise skin health first.
Healthy skin is a foundation for prosthetic success.
Ignoring this leads to repeated problems.
Some patients have very limited muscle control or balance.
A complex prosthesis may offer little benefit.
Prescribing in such cases raises false hope.
Sometimes, non-prosthetic aids provide more benefit.
Doctors should choose the least complex effective option.
More technology is not always better.
A prosthesis should reduce effort, not add to it.
If the effort outweighs benefit, prescription is not justified.
Using a prosthesis requires practice and care.
Without family or caregiver support, early use may fail.
Doctors must consider home environment.
Crowded spaces or poor hygiene conditions may affect use.
Prescribing without addressing these risks can harm outcomes.
Context matters deeply.
Sometimes, social solutions are needed before medical ones.
Ignoring context leads to poor adherence.
Some families push for immediate prescription due to fear of missing benefits.
This pressure should not override clinical judgement.
Timing must serve the patient, not anxiety.
An unused prosthesis is a heavy financial burden.
Doctors should protect families from unnecessary expense.
Ethical care includes cost awareness.
Clear plans reduce panic-driven decisions.
This improves trust and outcomes.
Some conditions improve with time.
Early prosthetic prescription may interrupt this process.
Observation can be an active choice.
Response to therapy reveals readiness.
Plateaus may later signal the right time.
Therapy guides timing.
Not prescribing now does not mean never.
Regular reassessment keeps options open.
Every prescription carries responsibility.
Harm includes physical, emotional, and financial damage.
Doctors must weigh all three.
Pressure may come from families, systems, or industry.
Clinical judgement must remain independent.
This protects trust.
A well-explained no builds respect.
Patients value honesty.
Communication matters as much as decision.
When a patient has already tried and rejected multiple devices, the reason must be understood before prescribing again.
Rejection is often blamed on motivation, but the cause may be pain, poor fit, or wrong timing.
Prescribing again without fixing the root issue usually leads to the same outcome.
Prosthetic use is not a one-day event. It requires regular follow-up, training, and adjustments.
If a patient cannot return for reviews due to distance, work pressure, or family issues, outcomes suffer.
In such cases, delaying or choosing simpler support may be safer.
Patients who consistently miss therapy or ignore care instructions struggle with prosthetic use.
This is not always intentional, but it affects results.
Doctors should stabilise routines before prescribing complex devices.
Conditions like uncontrolled diabetes, heart disease, or severe fatigue affect healing and tolerance.
A prosthesis adds physical demand to the body.
Prescribing during medical instability increases risk.
Rapid weight loss or gain changes socket fit and comfort.
Prescribing during unstable weight leads to repeated issues.
Waiting allows the body to stabilise.
Active infection anywhere in the body affects recovery.
Skin and tissue response becomes unpredictable.
Prosthetic prescription should wait until stability returns.
Children grow quickly, especially during certain ages.
A prosthesis prescribed during rapid growth may become unusable soon.
Frequent changes can frustrate both child and family.
Children may not always express discomfort or fear clearly.
Forcing use too early can create long-term resistance.
Play-based readiness should guide timing.
Parents often want quick solutions.
Doctors must guide families patiently.
Protecting the child’s long-term relationship with devices is critical.
Older adults may fatigue quickly.
A prosthesis that requires high effort may not be sustainable.
Prescribing without considering energy cost leads to abandonment.
Adding a device can change balance.
If fall risk is high, prosthetic use may be unsafe initially.
Stability must come first.
Mild memory issues can affect safe use.
Doctors should assess this carefully.
Sometimes, delaying or simplifying is the best care.
Some jobs require speed, precision, or endurance beyond prosthetic capacity.
Prescribing without aligning expectations causes disappointment.
Work counselling may be needed first.
Highly variable routines or heavy manual labor may not suit certain devices.
Doctors should match prescription to lifestyle.
Mismatch leads to non-use.
Dust, heat, and water exposure affect prosthetics.
If lifestyle includes these factors, timing and device choice matter.
Sometimes waiting or choosing alternatives is wiser.
High-end prosthetics are often seen as complete solutions.
In reality, they demand more training and care.
Prescribing based on technology appeal rather than readiness is risky.
Patients may come with fixed ideas from online content.
Doctors must reset expectations gently.
Prescription should follow understanding, not hype.
Newer is not always better.
Proven, simpler solutions often succeed more.
Clinical judgement must guide choice.
If a patient cannot describe what they want to do with the prosthesis, readiness is low.
Goals guide design and training.
Without them, use remains random.
Major life changes like relocation or job change affect needs.
Prescribing during uncertainty may miss the mark.
Waiting allows clarity.
Stable goals lead to better engagement.
Doctors should help patients articulate these first.
Sometimes therapy alone improves function enough.
This avoids unnecessary prescription.
Observation can be active care.
Slings, braces, or adaptive tools may meet current needs.
These can bridge gaps safely.
They buy time for better decisions.
Understanding options reduces anxiety.
Education itself can improve outcomes.
Not every solution is physical.
Patients accept decisions better when reasons are clear.
Vague explanations create doubt.
Transparency builds trust.
Not prescribing now does not mean stopping care.
Doctors should outline next steps.
This reduces fear.
Written plans provide clarity.
Review dates show commitment.
This keeps patients engaged.
Many successful users first experienced a delay.
Waiting improved readiness and acceptance.
These cases highlight the value of patience.
Avoiding early prescription prevented skin and joint issues.
Later fitting was smoother.
Outcomes improved.
Patients who had time to adapt emotionally often used devices more confidently.
Mental readiness mattered.
Timing protected this.
Good care is not about doing more.
It is about doing what is right at the right time.
Restraint is a skill.
Avoiding unnecessary devices protects dignity.
Patients value honesty over quick fixes.
Trust grows through careful choices.
Waiting does not mean failure.
In many cases, it is the reason success happens.
Timing and judgement define good prosthetic care.
Some patients arrive with a fixed belief that a prosthesis is the only path forward. This belief may come from fear, family pressure, or stories they have heard.
Even when pain is high or joints are unstable, they may push for immediate fitting.
In such cases, the doctor’s role is to slow the process and protect the patient from harm caused by haste.
There are patients who appear physically strong and motivated during short clinic visits.
However, longer observation may reveal fatigue, poor control, or emotional distress that only appears with time.
Prescribing based on first impressions alone can lead to poor outcomes.
Some patients agree to everything out of respect or fear of questioning authority.
They may not voice discomfort, confusion, or doubt.
Doctors must actively check understanding before prescribing.
A new lower-limb prosthesis changes balance and movement patterns.
If core strength and reaction time are poor, fall risk increases.
In such cases, waiting and strengthening first is safer.
When a prosthesis is heavy or hard to control, patients may overuse the other limb.
This leads to shoulder, wrist, or back pain.
Doctors should delay prescription until balanced use is possible.
Early skin injury creates fear and mistrust.
Even after healing, patients may avoid prosthetic use.
Preventing this first injury is critical.
Prosthetics are a major investment.
When a device is unused, the emotional and financial burden is heavy.
Doctors should protect families from avoidable loss.
A failed prosthetic experience can reduce trust in future recommendations.
Patients may resist even appropriate care later.
This long-term impact is often underestimated.
Patients may blame themselves for not using the device.
This can lower confidence and motivation.
Right timing protects self-belief.
Trials allow patients to experience devices without pressure.
They help assess comfort, control, and readiness.
Doctors should use trials wisely.
If pain, wounds, or fear are high, even trials may harm confidence.
Waiting protects the learning process.
Not every patient benefits from early exposure.
Trial outcomes provide valuable information.
They can confirm readiness or signal the need to wait.
This data-driven approach improves judgement.
Manufacturers see patients at close range.
They often notice discomfort or confusion early.
Responsible manufacturers support clinical restraint.
Good outcomes come from teamwork.
Manufacturers should support doctors when waiting is advised.
This builds long-term trust.
Patient education should replace persuasion.
Understanding leads to better decisions.
Ethical practice benefits everyone.
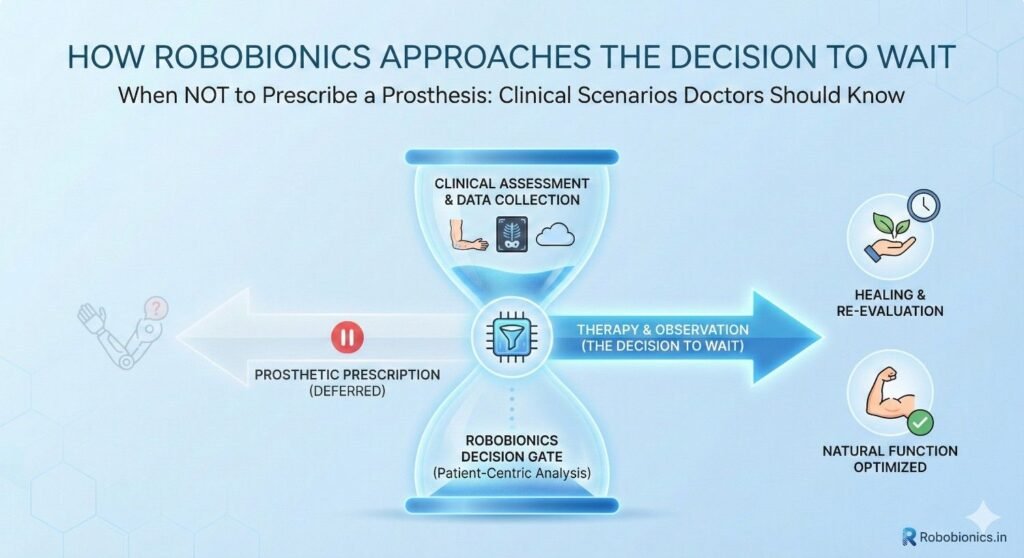
At Robobionics, success is measured by daily use, not delivery speed.
If a patient is not ready, waiting is recommended.
This protects outcomes.
Decisions are made with the care team.
Therapist feedback guides readiness.
Team alignment improves success.
Waiting does not mean inactivity.
Education, counselling, and basic training continue.
This prepares patients for later success.
Pain no longer dominates daily life.
Learning becomes possible.
This signals growing readiness.
No new wounds or swelling appear with regular movement.
The body handles load better.
This supports safe fitting.
Patients can describe what they want to do.
Goals guide device choice.
Clarity signals readiness.
Waiting should be explained as active preparation.
This changes perception.
Patients feel involved, not delayed.
Clear milestones reduce anxiety.
Patients know what they are waiting for.
This builds patience.
Involved patients accept decisions better.
Dialogue builds trust.
This strengthens outcomes.
Clear documentation protects both patient and doctor.
It also supports continuity of care.
Transparency matters.
Waiting without review feels like abandonment.
Planned follow-ups maintain engagement.
Care remains visible.
Plans should evolve with recovery.
Flexibility shows commitment.
Patients feel supported.
Medical training often focuses on action.
Restraint must be taught equally.
Knowing when not to act is critical.
Real cases teach better than rules.
Reflection builds judgement.
Experience deepens understanding.
Senior guidance improves decision-making.
Team discussion reduces error.
Learning is continuous.
Delayed fitting often leads to smoother adaptation.
Success is seen later.
This confirms the value of waiting.
Fewer skin issues and less abandonment occur.
Long-term use improves.
These outcomes matter.
Honest decisions build trust.
Patients return with confidence.
This is success too.
Speed does not equal quality.
Thoughtful timing defines expertise.
Patients benefit from patience.
Saying no protects bodies, minds, and futures.
It requires courage and clarity.
This is true clinical care.
When prescribed at the right moment, prosthetics restore dignity and function.
Waiting ensures that moment is not missed.
This is the wisdom every clinician should carry.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body