
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Before a prosthesis can restore movement, the limb must be alive with good blood flow. This truth is simple, yet often overlooked in the rush to refer patients for prosthetic fitting. Vascular health decides whether wounds heal, skin survives pressure, and sockets feel comfortable or painful. When blood supply is poor, even the best prosthesis will fail. When blood supply is optimized, healing becomes predictable and function follows.
This article is written for clinicians who manage patients before prosthetic referral, especially those with diabetes, vascular disease, or trauma. It explains how to assess circulation using tools like ABI and Doppler, how to interpret findings in real practice, and how to act on them to improve healing. The focus is practical and grounded in everyday clinical settings across India, where early vascular decisions shape long-term prosthetic success.
Every stage of recovery after amputation depends on blood flow. Oxygen and nutrients reach the wound only through healthy vessels. When circulation is weak, healing slows and tissue becomes fragile.
A limb that looks healed on the surface may still have poor deep circulation. This hidden weakness shows up later as skin breakdown inside the socket.
Doctors should treat blood flow as the base on which all prosthetic success rests.
Poor blood flow reduces skin strength and tolerance to pressure. Even gentle socket contact can cause redness, pain, or open wounds.
Patients with weak circulation often struggle with repeated adjustments and long gaps between fittings. Frustration builds quickly.
Optimizing circulation early prevents these setbacks and protects patient confidence.
Many patients do not report classic symptoms like rest pain or color change. Reduced sensation hides warning signs.
Basic wound closure may mislead clinicians into assuming readiness. Without objective testing, circulation problems remain unseen.
Structured vascular assessment prevents these oversights.
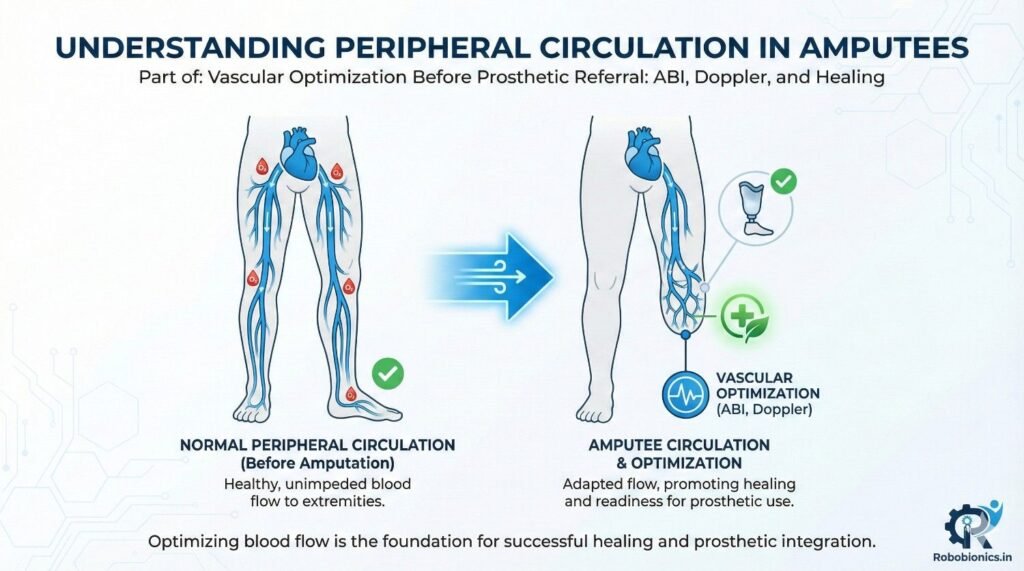
Amputation alters blood flow patterns. Some vessels are removed, while others take on increased load.
Swelling and surgical trauma further affect circulation in early stages. This makes clinical judgment difficult without testing.
Doctors should expect change and reassess flow over time.
Arterial disease limits blood reaching tissues. This causes slow healing, cool skin, and pain with pressure.
Venous problems affect blood return. Swelling and skin congestion are common.
Both impact prosthetic tolerance but require different management approaches.
Diabetes damages small blood vessels and masks symptoms through nerve loss. Circulation may be poor even when pulses feel present.
Visual assessment alone is unreliable in these patients.
Objective testing is essential before prosthetic referral.
The ankle-brachial index compares blood pressure at the ankle to that in the arm. It gives a snapshot of large vessel blood flow.
A normal ratio suggests adequate circulation. Lower values point to blockage or narrowing.
This simple test offers valuable early guidance.
ABI works best in patients without severe vessel calcification. It is a good screening tool in many adults.
For patients with clear results, it helps decide whether further testing is needed.
Doctors should use it as a starting point, not a final answer.
In diabetic and elderly patients, vessels may be stiff and give falsely high readings. A “normal” ABI can still hide poor flow.
Clinicians should correlate ABI with wound healing and skin signs.
Doubt should lead to Doppler or further studies.
Doppler ultrasound shows blood flow patterns, not just pressure. It helps identify where flow is reduced.
This detail is crucial when planning healing timelines and prosthetic referral.
Doppler adds clarity when ABI results are unclear.
Healthy vessels show smooth, strong waveforms. Flattened or weak signals suggest compromised flow.
Doctors do not need to master technical details, but should understand basic patterns.
Clear reports support better decisions.
Doppler is indicated when wounds heal slowly, skin looks fragile, or ABI is unreliable.
It is especially valuable before referring high-risk patients for prosthetics.
Early use prevents trial-and-error care.
A closed wound does not always mean healed tissue. Deep layers may still lack adequate blood supply.
These tissues fail under socket pressure, leading to breakdown.
Doctors should assess healing quality, not just closure.
Warm skin, healthy color, and gradual hair regrowth suggest better circulation. Stable healing without repeated breakdown is another sign.
These signs should match objective test results.
Mismatch signals risk.
Patients with adequate circulation usually tolerate shaping and early socket trials well.
Those with poor flow struggle despite good technique.
Vascular findings help predict these outcomes.
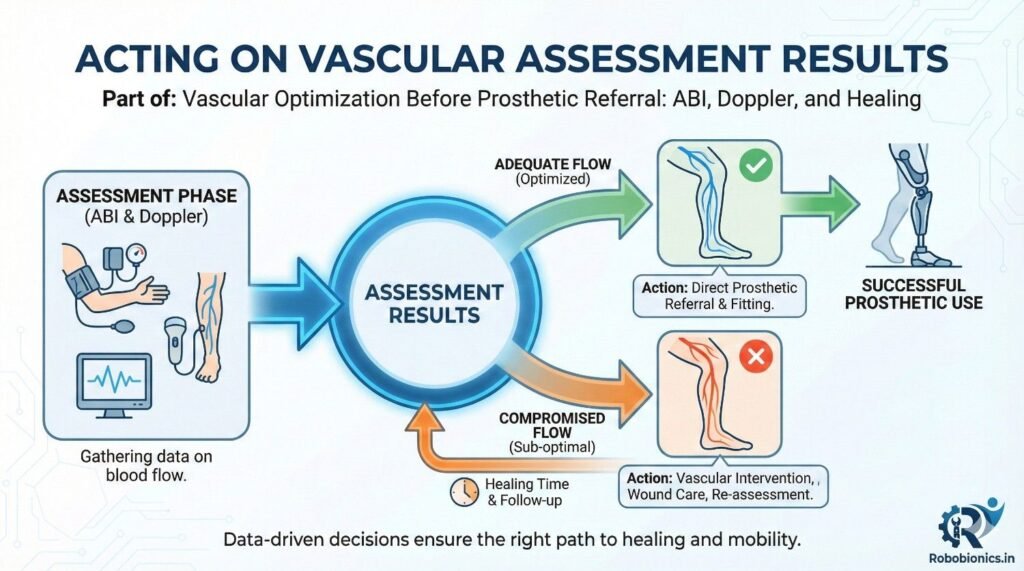
If tests and clinical signs suggest good flow, prosthetic referral can proceed confidently.
Doctors should still monitor changes, especially in early fitting.
Even good circulation can fluctuate.
Borderline results call for caution. Delaying referral while improving circulation may save time later.
Interventions may include medical management or referral to vascular specialists.
Clear communication with patients is essential.
Poor circulation requires correction before prosthetic referral. Fitting a socket in this state risks failure.
Doctors should prioritize limb survival and healing over speed.
Protecting tissue protects long-term function.
When vascular tests show reduced blood flow, early medical action can make a meaningful difference. Simple steps like adjusting blood pressure control, managing cholesterol, and improving blood sugar stability often improve tissue perfusion over time.
Doctors should review current medications carefully. Some patients may be undertreated or inconsistently treated due to fragmented care.
Small improvements in circulation can change healing outcomes and prosthetic readiness.
Medicines that improve blood flow or reduce clot risk support healing in patients with arterial disease. These are not quick fixes, but they create a better environment for tissue repair.
Doctors should explain to patients that these medicines support long-term limb health, not just immediate symptoms.
Adherence improves when patients understand the purpose.
Smoking is one of the strongest blockers of healing. Even small amounts reduce blood flow and oxygen delivery.
Nutrition, hydration, and gentle activity also affect circulation. Patients often underestimate their impact.
Doctors should address these factors kindly but clearly, linking them directly to prosthetic success.
Some patients show poor circulation despite best medical care. In these cases, further intervention may be required.
Delaying referral for evaluation wastes valuable healing time. Early vascular consultation often preserves limb potential.
Doctors should not wait for repeated wound failure before acting.
Revascularization restores blood flow by opening or bypassing blocked vessels. This can be done through minimally invasive procedures or surgery.
Improved flow often leads to visible changes in skin warmth and healing speed.
Doctors should set realistic expectations while emphasizing benefits.
After circulation improves, tissues need time to stabilize. Immediate prosthetic referral may still be premature.
Doctors should reassess healing trends, not just test results. Stable improvement over weeks is a good sign.
This patience prevents repeated setbacks.
Circulation can improve or worsen over time. One test result does not guarantee future stability.
Regular reassessment catches problems early. This is especially important during shaping and compression.
Doctors should plan follow-up intervals based on risk level.
Objective tests guide decisions, but clinical signs confirm reality. Skin response to compression and activity reveals true tolerance.
Doctors should trust both data and observation.
Balanced judgment leads to safer referral.
New pain, color change, or delayed healing after initial progress should raise concern.
These signs often appear before major breakdown occurs.
Early action preserves gains already made.
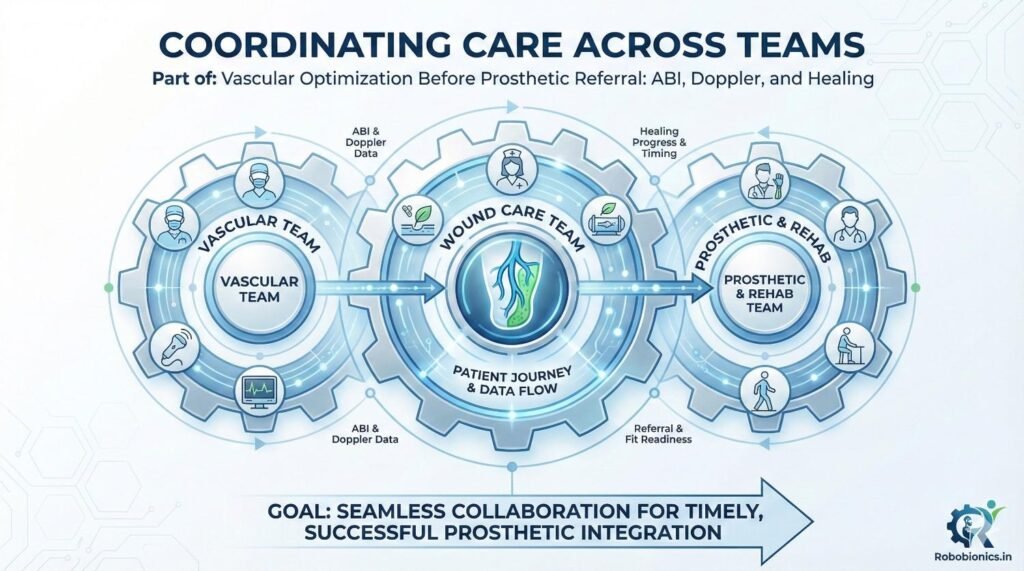
Clear communication ensures that prosthetic timelines align with vascular recovery. Specialists need to know functional goals, not just wound status.
Shared understanding reduces conflicting advice.
Doctors should actively coordinate rather than refer and wait.
Therapists should know circulation limits to adjust activity and compression safely.
Overloading fragile tissue can undo vascular gains.
Team alignment protects healing.
Early prosthetist input helps plan realistic timelines and socket strategies.
However, fitting should wait until circulation supports pressure tolerance.
Clear handover prevents frustration on all sides.
Diabetic patients often have mixed arterial and microvascular disease. Standard tests may underestimate risk.
Healing may look slow but steady. Doctors should avoid rushing referral.
Extra caution improves long-term use.
Age-related vessel stiffness and skin fragility increase risk. Healing may require longer observation.
Doctors should prioritize comfort and safety over speed.
Realistic planning builds trust.
Trauma patients may have localized vessel damage. Circulation may be uneven across the limb.
Targeted assessment prevents missed risk areas.
Individualized care works best.
A prosthetic socket applies repeated pressure. Without good blood flow, tissue breaks down.
Doctors should imagine the limb under daily load, not just at rest.
This perspective guides safer decisions.
Compression and shaping act as early stress tests. Limbs with adequate flow adapt gradually.
Poor tolerance signals need for further optimization.
Doctors should respect these signals.
The right time is when circulation is stable, healing is consistent, and tissue tolerates pressure.
This moment varies by patient.
Judgment matters more than timelines.
Patients referred at the right time experience fewer breakdowns and fewer clinic visits.
This saves resources and improves satisfaction.
Early care pays off later.
Good circulation supports skin health and comfort. Patients wear their prosthesis longer and more confidently.
This improves mobility and quality of life.
Doctors see the difference over time.
Repeated failures erode patient trust. Thoughtful vascular optimization protects dignity.
Patients feel cared for, not rushed.
This is good medicine.
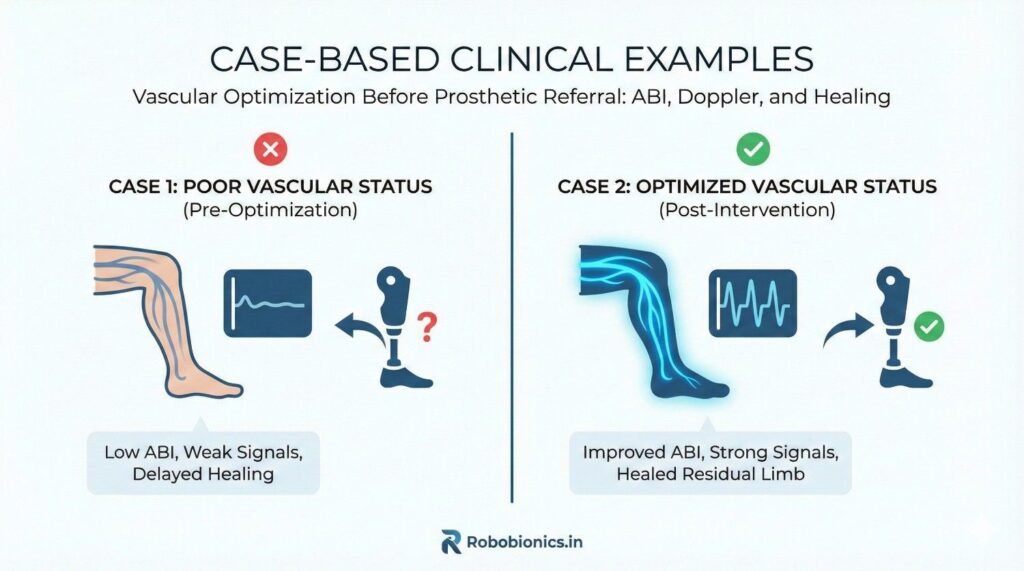
A patient with long-standing diabetes had a below-knee amputation that appeared to heal on time. The wound closed, and swelling reduced with compression. However, early socket trials caused redness and pain within minutes.
ABI was borderline, and Doppler showed weak distal flow. Medical optimization and smoking cessation were started, followed by vascular consultation. Over the next weeks, skin warmth improved and compression tolerance increased.
When prosthetic referral resumed, fitting progressed smoothly. This case shows how early vascular review prevents repeated failure.
An elderly patient had a near-normal ABI but slow healing and cool skin. Doppler revealed calcified vessels and poor waveform quality.
Relying on ABI alone would have led to early referral and breakdown. With Doppler-guided caution and extended healing time, the limb stabilized.
Objective testing paired with clinical signs avoided harm.
A trauma patient had uneven circulation due to localized vessel damage. One area healed well, while another remained fragile.
Targeted care and delayed pressure over the weak zone allowed gradual adaptation. Prosthetic design accounted for circulation differences.
Individualized planning led to success.
Wound closure is an important milestone, but it is not the finish line. Deep tissue health and circulation decide tolerance.
Doctors who refer based on closure alone often see repeat breakdowns.
Healing quality matters more than speed.
ABI or Doppler alone cannot tell the full story. Each test has limits, especially in diabetes and old age.
Mismatch between tests and clinical signs should prompt reassessment.
Balanced interpretation prevents errors.
Patients may report coldness, fatigue, or discomfort before visible signs appear. These symptoms often reflect circulation limits.
Dismissing them delays intervention.
Listening saves time and tissue.
A clear flow helps busy clinics. Start with clinical exam and history, add ABI, then Doppler if needed.
This stepwise approach uses resources wisely.
Consistency improves outcomes.
Clinics should define when to pause referral and optimize circulation. Clear thresholds reduce confusion.
Doctors can still apply judgment within structure.
Clarity supports teamwork.
Recording test results, skin signs, and healing trends builds a useful timeline.
This helps future decisions and referrals.
Good notes support continuity.
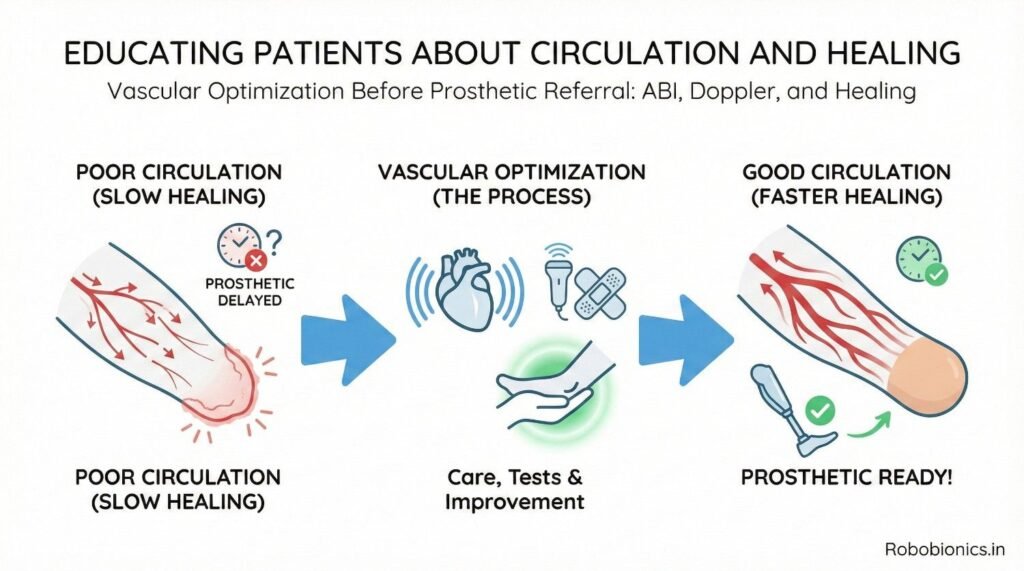
Patients understand better when told that blood brings food and oxygen to the limb. Without it, skin cannot stay strong.
Simple explanations reduce fear and improve cooperation.
Education should be repeated gently.
Patients are more motivated when they see how habits affect walking and comfort. Smoking cessation and diet changes feel meaningful when linked to function.
Doctors should use this connection often.
Motivation improves adherence.
Honest timelines prevent frustration. Patients accept delay better when they understand the reason.
Shared planning builds trust.
Trust supports healing.
Stable skin without repeated redness or wounds shows readiness. This matters more than calendar dates.
Doctors should celebrate these signs with patients.
Positive feedback builds confidence.
Limbs that tolerate shaping and light activity without pain usually tolerate sockets well.
These functional signs guide safe referral.
Function predicts success.
True success shows months later, when patients use their prosthesis daily without breakdown.
Early vascular care supports this outcome.
Good beginnings last longer.
Optimizing circulation is not an optional step. It is a core responsibility before prosthetic referral.
Doctors who embrace this role reduce suffering.
Care improves outcomes.
Rushing referral feels helpful but often delays true recovery. Thoughtful pacing protects tissue and dignity.
Safety builds confidence.
Confidence restores mobility.
When clinicians, vascular teams, rehab specialists, and prosthetists align, patients heal better and walk sooner.
Blood flow supports every step.
This is how prosthetic success begins.
At the first post-operative or pre-referral visit, clinicians should assess skin color, temperature, capillary refill, and wound behavior. These simple observations often reveal more than numbers alone.
A brief history should include rest pain, night pain, cold sensitivity, and prior vascular procedures. Even mild symptoms matter in high-risk patients.
This screening sets the direction for further testing.
If clinical signs are reassuring, ABI can be used as an initial screen. When ABI is low, borderline, or does not match the clinical picture, Doppler should follow.
In diabetic and elderly patients, Doppler should be considered early due to unreliable ABI results.
Clear decision points reduce delay and confusion.
Before prosthetic referral, clinicians should ask whether the limb tolerates compression, shows stable healing, and maintains skin integrity with daily activity.
If the answer is uncertain, referral should pause. Optimizing circulation at this stage prevents failure later.
This pause is protective, not restrictive.
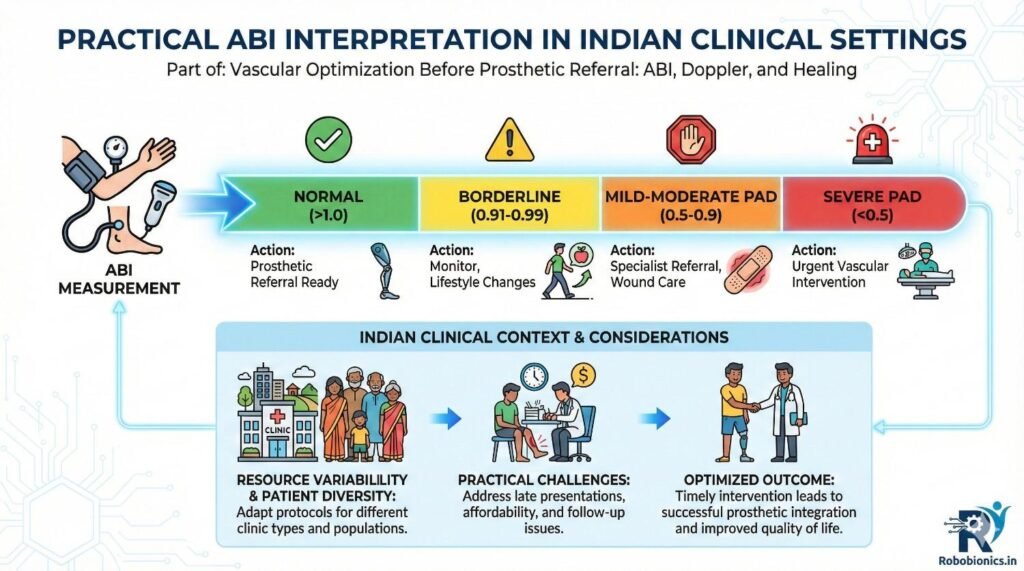
An ABI in the normal range suggests adequate large-vessel flow, but does not guarantee healing capacity. Functional tolerance must confirm it.
Low ABI values signal higher risk, but improvement trends matter. A rising ABI with better skin signs is encouraging.
Clinicians should think in patterns, not absolutes.
Calcified vessels common in diabetes and aging may produce high ABI readings. These readings can mislead inexperienced clinicians.
When ABI is high but skin is cool or healing is slow, Doppler becomes essential.
Questioning numbers is part of good care.
ABI should inform decisions, not replace judgment. It works best when paired with Doppler, wound behavior, and patient feedback.
Rigid reliance on ABI alone often leads to errors.
Context always matters.
Clinicians should focus on flow presence, waveform quality, and symmetry. These elements give a clear sense of circulation strength.
Poor or flattened waveforms suggest limited pressure tolerance even if wounds look closed.
Understanding these basics improves referral timing.
If reports are vague, clinicians should ask for clarification. Knowing whether flow is monophasic or weak helps guide care.
Clear communication improves report usefulness.
Doctors should feel comfortable seeking detail.
Doppler findings help anticipate how much pressure tissue can tolerate. This guides both referral timing and socket strategy.
Better planning reduces trial-and-error fitting.
Data supports foresight.
In patients with good circulation, wound healing and shaping progress steadily. Compression tolerance improves week by week.
Prosthetic referral is often safe once stability is observed over time.
Patience still matters, even in good cases.
Patients with vascular disease may need longer observation. Healing may appear slow but consistent.
Rushing these cases leads to breakdown and re-referral.
Doctors should normalize longer timelines early.
High-risk patients benefit from closer follow-up. Repeating clinical exams and Doppler at intervals guides decisions.
Structured reassessment prevents surprises.
Planning improves confidence.
Prosthetists should know where circulation is weakest. This helps guide socket relief areas and load distribution.
Clear handover improves design choices.
Silence creates avoidable problems.
In borderline circulation, conservative designs protect tissue. Advanced suspension can wait until tolerance is proven.
Staged progression reduces breakdown risk.
Gradual loading works best.
Early prosthetic use should be closely monitored. Any redness or pain should trigger immediate review.
Quick response preserves progress.
Delay compounds damage.
Proper vascular optimization reduces repeated fittings, wound care visits, and hospital readmissions.
This saves time for clinicians and patients alike.
Efficiency improves care quality.
Patients who experience fewer setbacks trust their care team more. Trust improves adherence and outcomes.
Early vascular care builds this trust.
Trust sustains recovery.
Clear vascular pathways reduce variation in outcomes. Standard care protects patients regardless of location.
Consistency is equity.
Equity improves public health.
Blood flow decides healing. Healing decides prosthetic success. Skipping vascular optimization risks everything that follows.
Tests guide, but clinical signs confirm.
Balance speed with safety.
Add structured vascular checks before referral. Question mismatches between tests and tissue behavior.
Pause when unsure and optimize first.
Small changes bring big results.
Early vascular care protects skin, comfort, and dignity. Patients walk longer, with fewer setbacks.
This is how good outcomes are built.
One careful decision at a time.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body