
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation



Age changes the body, but it does not take away the need for independence, dignity, or movement.
For older adults who need a prosthesis, success depends on more than just fit and technology. It depends on strength, balance, skin health, confidence, and daily habits that are very different from those of younger users.
In geriatric care, frailty is not a weakness. It is a signal.
It tells us how much load the body can handle, how fast it can adapt, and how carefully each step must be planned.
At Robobionics, we have worked closely with elderly prosthetic users across India, from active seniors to those with limited mobility. One lesson stands out clearly. Standard prosthetic protocols do not work well for frail patients. They need adjusted timelines, gentler goals, and smarter support systems.
This article focuses on frailty-adjusted protocols for prosthetic use in geriatric patients. We will explain what frailty really means, how it affects prosthetic outcomes, and what physicians, prosthetists, caregivers, and families can do to improve safety and success.
The goal is simple.
To help older adults use prosthetics comfortably, confidently, and for the long term.
Frailty does not mean weakness alone, and it does not affect all elderly people in the same way.
Some older adults remain strong and active, while others lose strength, balance, and energy much faster.
Frailty is about how much stress the body can handle before it starts to struggle.
This stress can come from walking, lifting, wearing a socket, or even standing for long periods.
Understanding frailty helps clinicians choose safer and more realistic prosthetic plans.
Frailty often appears as slow walking, easy tiredness, or fear of falling.
Small tasks may take more effort than before.
Many elderly patients avoid movement because they feel unsure or unsafe.
This reduces strength even more and creates a cycle that is hard to break.
A prosthetic plan must work within these limits, not ignore them.
A frail body adapts slowly to new loads and movements.
Muscles take longer to strengthen, and balance improves at a slower pace.
If standard prosthetic goals are applied without adjustment, the risk of falls, pain, and skin injury increases.
This often leads to early rejection of the prosthesis.
Frailty-aware planning improves comfort, safety, and long-term use.
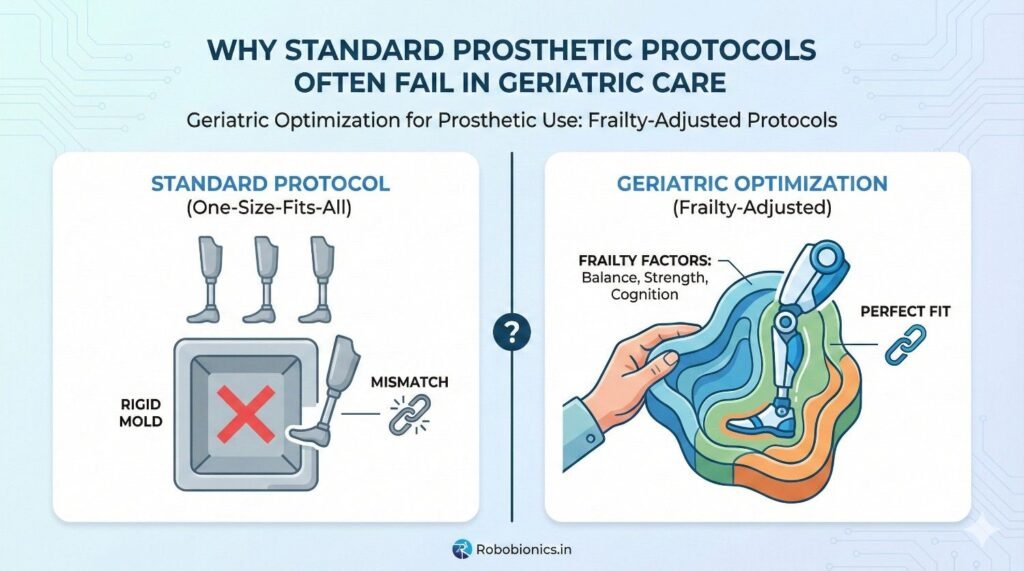
Many prosthetic protocols are built around younger or middle-aged users.
They assume good balance, fast healing, and high activity tolerance.
When these same plans are applied to frail elderly patients, the body cannot keep up.
This creates stress instead of progress.
Older users need protocols that match their pace, not someone else’s.
Rushing prosthetic training in elderly users often leads to pain, fear, and loss of trust.
A single fall can undo weeks of progress.
When patients feel unsafe, they stop trying.
Once confidence is lost, it is very hard to regain.
Slower progress with fewer setbacks often leads to better final outcomes.
Many elderly users stop using their prosthesis within the first few months.
The reasons are often physical strain, discomfort, or fear of injury.
These are not failures of motivation.
They are signs that the plan was not suited to the patient’s body.
Frailty-adjusted care directly addresses these issues.
Age alone does not define frailty.
Two people of the same age can have very different abilities.
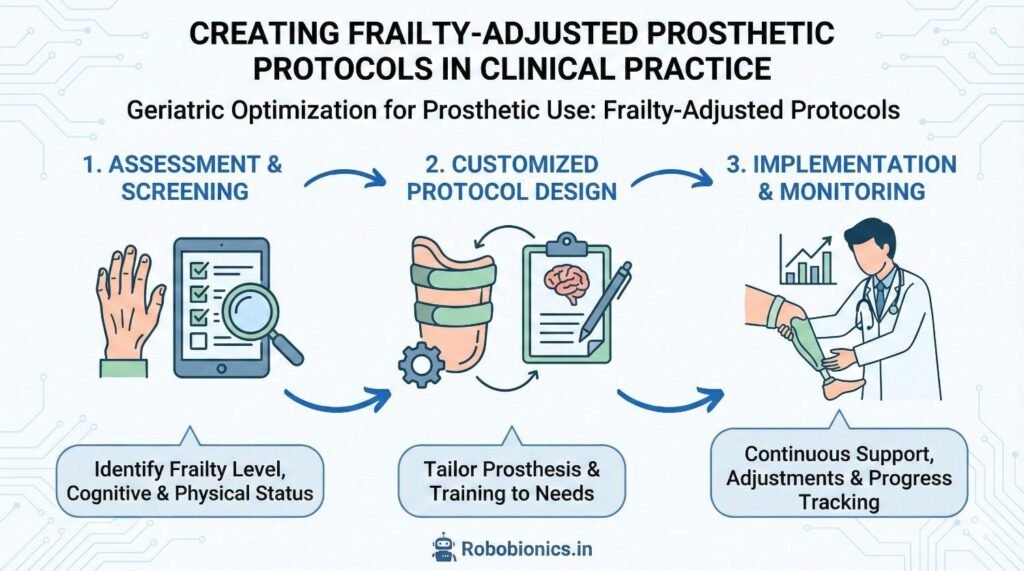
Physicians should assess strength, balance, endurance, and daily function.
Simple observations during walking or standing can reveal a lot.
This assessment guides safer prosthetic decisions.
Frail patients often have limited energy reserves.
Tasks that seem simple may leave them exhausted.
Prosthetic use requires extra energy, especially in the early stages.
Ignoring this can lead to frustration and overuse injuries.
Energy limits must shape training duration and intensity.
Many elderly patients rely on family members or caregivers.
Their role is critical in daily prosthetic use.
Caregivers can provide insight into daily challenges and routines.
Their involvement improves safety and consistency.
Planning without them often leads to gaps in care.
For younger users, success may mean long walking distances or full-day use.
For elderly users, success often looks different.
Standing safely, moving indoors, or performing basic daily tasks may be the main goals.
These outcomes still restore dignity and independence.
Clear goal setting prevents disappointment and builds confidence.
Prosthetic goals should reflect how the patient actually lives.
A home-based user needs different outcomes than someone who goes outdoors often.
Understanding daily routines helps prioritize the right movements.
This makes training more meaningful and practical.
Goals should support life, not impress on paper.
Frailty levels can change with health, illness, or recovery.
Goals should remain flexible.
What feels impossible today may become achievable later.
Likewise, goals may need adjustment after health setbacks.
A flexible approach supports long-term use.
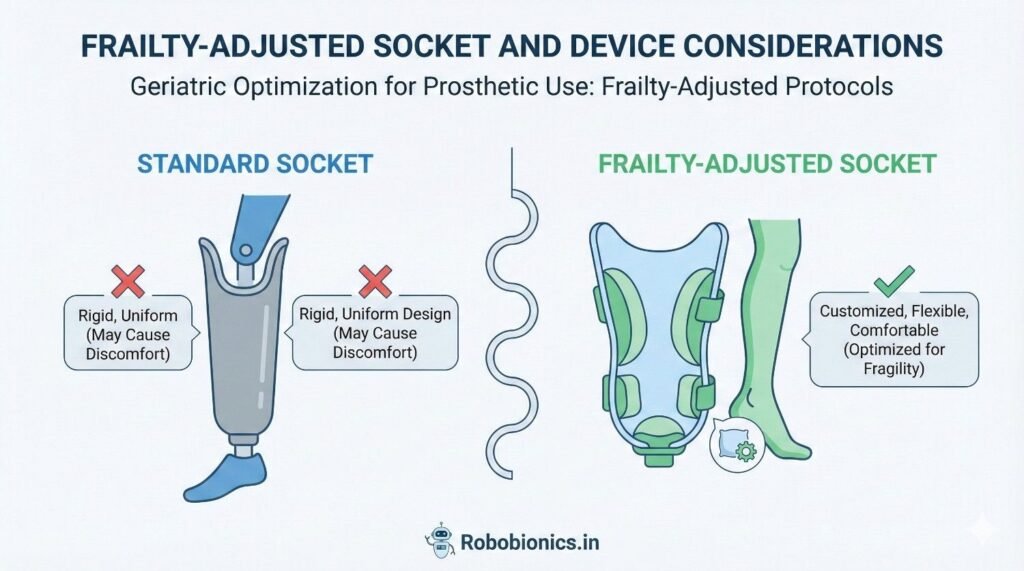
Elderly users often value comfort more than advanced features.
A simple, reliable prosthesis is easier to accept and use.
Heavy or complex systems may increase fatigue and confusion.
This reduces daily use.
Comfort-driven design improves compliance and safety.
Even small increases in weight can feel heavy to a frail user.
Poor balance magnifies this effect.
Lightweight components and stable alignment reduce strain.
They also lower the risk of falls.
Design choices should always respect physical limits.
Putting on and removing a prosthesis can be challenging for elderly users.
Limited hand strength, vision issues, or joint stiffness make this harder.
Simpler suspension systems and clear markings help.
If a prosthesis is hard to use, it will not be used.
Ease of handling is a key success factor.
Rehabilitation should move at a pace the body can handle.
Shorter sessions with proper rest are often more effective.
Pushing too hard leads to pain and fear.
Gentle progress builds trust and consistency.
Quality matters more than speed.
Before advanced movements, basic balance must be addressed.
Standing safely is more important than walking far.
Balance training reduces fall risk and builds confidence.
Confidence encourages continued use.
Safety-first training protects both body and mind.
Frail patients benefit from repetition, but not from strain.
Simple movements practiced often work best.
Therapists should watch closely for signs of fatigue.
Stopping early is better than pushing through exhaustion.
Respecting limits builds long-term strength.
Many elderly patients fear falling or getting hurt.
This fear often limits effort more than physical weakness.
Acknowledging fear openly helps reduce it.
Ignoring it makes it stronger.
Confidence grows when patients feel understood.
Small improvements matter a lot in geriatric care.
Standing longer or taking a few safe steps is progress.
Recognizing these moments boosts motivation.
It reminds patients that effort leads to results.
Positive reinforcement supports continued use.
Encouragement from family builds emotional safety.
It also increases consistency in practice.
When families understand realistic goals, pressure reduces.
This creates a healthier recovery environment.
Support systems are part of the protocol.
Health conditions, medications, and activity levels change with age.
Prosthetic needs change with them.
Regular follow-ups allow early adjustments.
This prevents discomfort and breakdown.
Ongoing care is essential, not optional.
Elderly skin is fragile and heals slowly.
Even small issues need attention.
Energy levels should also be reviewed regularly.
Fatigue often signals the need for adjustment.
Listening early prevents bigger problems later.
Sometimes reducing usage goals improves overall success.
Using the prosthesis for specific tasks may be enough.
There is no single right way to succeed.
Success looks different for every elderly user.
Flexibility supports dignity and independence.
Frailty-adjusted prosthetic care begins with accepting that elderly patients cannot be managed using fixed rules or rigid timelines.
Each patient brings a unique mix of strength, fear, health conditions, and life context that must shape every clinical decision.
When protocols are flexible, clinicians can respond to the patient’s real abilities instead of forcing progress that looks good on paper.
This shift reduces failure rates and improves long-term acceptance.
Frailty-aware care is not about lowering standards, but about applying smarter standards.
In frail patients, tolerance matters more than targets.
How much standing, walking, or wearing time the body can safely handle should guide planning.
Daily tolerance often changes based on sleep, nutrition, or minor illness.
Protocols must allow adjustment without guilt or pressure.
When tolerance leads planning, patients feel safer and more willing to try.
Recovery time is not wasted time in geriatric care.
It is a necessary part of adaptation.
Muscles, joints, and skin need longer recovery after activity.
Ignoring this leads to soreness, fear, and withdrawal.
Planned rest improves consistency and reduces setbacks.
Poor nutrition weakens muscles, slows healing, and reduces energy.
Many elderly patients eat less due to appetite loss, dental issues, or illness.
Without enough protein and fluids, prosthetic training becomes much harder.
The body simply does not have the resources to adapt.
Addressing nutrition early improves every other outcome.
Even small gains in strength can improve balance and confidence.
Chair rises, supported standing, and light resistance exercises matter greatly.
Strength training does not need to be intense to be effective.
Consistency matters more than difficulty.
Stronger muscles protect joints and reduce fall risk.
Medications, chronic illness, and pain management all affect prosthetic use.
Coordination with physicians ensures safer training.
Adjusting therapy on days of low energy or pain prevents harm.
Ignoring medical factors often leads to failure.
Integrated care supports frail patients best.
Aging skin becomes thinner, drier, and less elastic.
It tears easily and heals slowly.
Inside a prosthetic socket, this skin faces pressure and friction daily.
Without protection, breakdown is common.
Skin care must be proactive, not reactive.
Socket design should spread pressure gently across stronger areas.
Sharp edges or tight spots must be avoided.
Wear time should increase slowly, allowing skin to adapt.
Early signs of redness should be taken seriously.
Prevention is always easier than healing.
Elderly users may not feel early pain clearly.
Visual skin checks become very important.
Patients and caregivers should inspect the limb every day.
Any change should be reported early.
Education turns patients into protectors of their own skin.
Fear of falling is common and reasonable in elderly patients.
A fall can cause serious injury and loss of confidence.
This fear often limits effort more than physical weakness.
Ignoring it reduces participation.
Addressing fear openly improves cooperation.
Training should focus first on stable standing and safe transfers.
Walking distance is less important initially.
Use of parallel bars, walkers, or hand support is not a failure.
It is a safety strategy.
Stability builds confidence, which supports progress.
Many falls happen at home, not in clinics.
Uneven floors, poor lighting, and loose rugs increase risk.
Clinicians should discuss home safety early.
Small changes can prevent serious injury.
A safe environment supports prosthetic use.

Elderly patients often depend on family for daily support.
Caregivers influence routine, safety, and motivation.
Including them in training improves understanding and consistency.
They help reinforce correct use and skin care.
Caregiver education is essential, not optional.
Families sometimes push patients to do more, faster.
This often comes from love, not understanding.
Clear communication helps families support safely.
Realistic goals reduce stress for everyone.
Support works best when expectations match reality.
Progress in frail patients is often slow and uneven.
Encouragement matters greatly.
Positive reinforcement builds confidence and trust.
Criticism or comparison harms motivation.
Emotional safety supports physical progress.
Success in elderly prosthetic care is not measured by speed or distance.
It is measured by safety, comfort, and regular use.
Being able to stand, move indoors, or perform daily tasks may be enough.
These outcomes restore dignity and reduce dependence.
Success must be defined with the patient, not for them.
A prosthesis that improves confidence and reduces fear has value.
Even limited use can improve quality of life.
Pushing for high performance at the cost of comfort often leads to rejection.
Balance is key.
Quality of life should guide decisions.
Short-term progress means little if the prosthesis is abandoned later.
Sustainable use is the true goal.
Frailty-adjusted protocols focus on long-term acceptance.
This approach leads to steadier outcomes.
Slow success often lasts longer.
In India, many elderly patients live with family and have limited access to therapy centers.
Home-based routines become very important.
Protocols must fit real living conditions.
Plans that ignore this often fail.
Practical care works better than ideal care.
Affordable, durable prosthetic solutions matter greatly.
Complex systems may be hard to maintain.
Simple designs with clear benefits are often more successful.
Ease of repair and use supports continuity.
Affordability supports long-term use.
Elderly patients value dignity deeply.
Being able to move independently, even in small ways, matters.
Care plans should respect personal values and comfort.
Listening builds trust and cooperation.
Dignity is a core outcome.
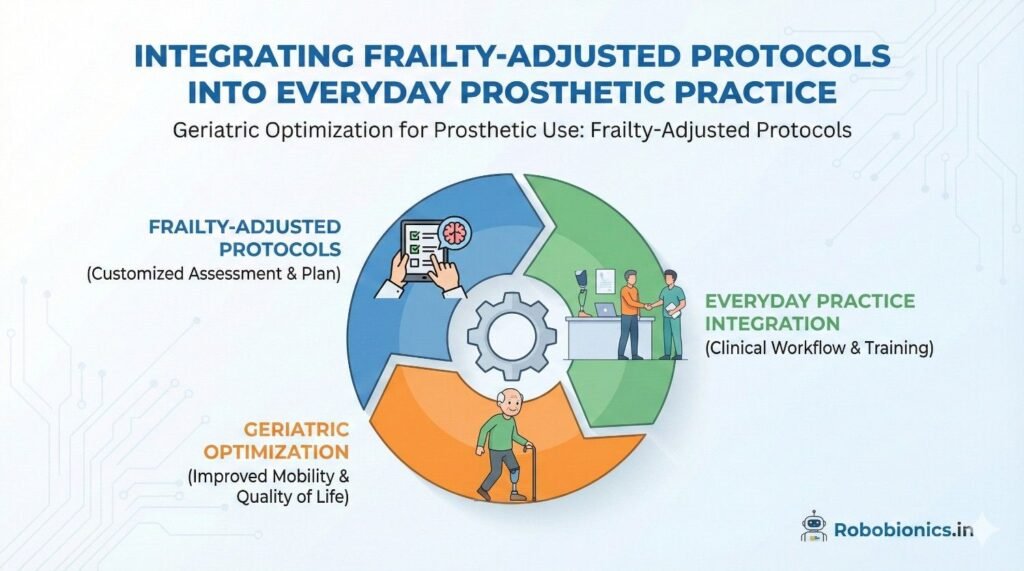
Frailty-adjusted care works best when it is built into everyday clinical systems rather than treated as an exception.
Appointment schedules, therapy plans, and follow-up routines must allow enough time for slow movement, rest, and patient questions.
When clinics reduce time pressure, elderly patients feel safer and more respected.
This comfort leads to better communication and more honest feedback.
Systems that allow gentle progress prevent burnout for both patients and clinicians.
Every member of the care team should understand how frailty affects prosthetic use.
This includes physicians, prosthetists, therapists, and support staff.
When teams share the same mindset, care becomes consistent and predictable.
Mixed messages often confuse patients and reduce trust.
Frailty-first thinking improves coordination and outcomes.
Measurements and assessments are useful, but they should never replace listening.
Elderly patients often express concerns in subtle ways.
Body language, hesitation, or silence can reveal discomfort.
Clinicians must remain attentive beyond checklists.
Human awareness is as important as clinical data.
Advanced technology is helpful only if the user feels safe using it.
For frail patients, reliability matters more than features.
Simple controls, predictable movement, and stable responses build trust.
Unpredictable behavior increases fear.
Confidence drives regular use.
Frail users tire easily, and heavy systems increase strain.
Lightweight designs reduce effort and improve balance.
Maintenance should be simple and affordable.
Complex upkeep often leads to device abandonment.
Technology must fit the user’s capacity, not challenge it.
Some elderly users benefit from devices that provide extra support.
Others prefer minimal assistance to feel in control.
Finding this balance requires open discussion.
Too much assistance can feel restrictive.
Personal preference should guide final choices.
Some elderly patients experience memory or attention issues.
This affects learning and routine formation.
Instructions may need repetition and simplification.
Written or visual cues often help.
Acknowledging cognitive change improves safety.
Complex steps increase confusion and error risk.
Simpler routines improve consistency.
Clear markings, consistent schedules, and limited choices support learning.
Caregivers play an important role here.
Simplicity protects independence.
Cognitive changes may progress slowly.
Regular review ensures continued safe use.
When safety concerns arise, plans must adapt.
This may include supervision or reduced use.
Ongoing monitoring protects dignity and well-being.
In some cases, the physical or cognitive load of prosthetic use may be too high.
This is a difficult but necessary discussion.
Choosing not to prescribe a prosthesis can sometimes protect quality of life.
Mobility aids may offer safer alternatives.
Ethical care prioritizes well-being over expectation.
Decisions should never be made in isolation.
Patients and families must be part of the conversation.
Clear explanations help everyone understand risks and benefits.
Shared decisions reduce regret and conflict.
Respect builds trust even in difficult moments.
Health and ability change with time.
What is not suitable today may become possible later, or vice versa.
Regular reassessment keeps care aligned with reality.
Flexibility is a strength, not weakness.
Ethical care is dynamic care.
Regular follow-up helps catch small issues early.
This includes skin changes, fatigue, or fear.
Early action prevents withdrawal from prosthetic use.
Consistency supports long-term success.
Follow-up is care, not maintenance.
Elderly patients often face health setbacks.
Prosthetic use may need adjustment during these times.
Temporary changes are not failures.
They protect recovery and confidence.
Support during setbacks builds resilience.
Even limited use can maintain strength and confidence.
Encouragement matters greatly.
Patients should feel supported, not judged.
Positive reinforcement sustains effort.
Engagement is a long-term goal.

When prosthetic care respects frailty, patients feel safer and more capable.
This safety allows confidence to grow slowly and naturally.
Confidence leads to regular use and better quality of life.
It cannot be rushed or forced.
Frailty-aware care meets patients where they are.
Geriatric prosthetic success is built on patience, planning, and respect.
Small steps taken carefully lead to lasting outcomes.
Rushed care often fails, while thoughtful care endures.
This truth is seen again and again in practice.
Time invested early saves effort later.
At Robobionics, we believe prosthetic care should always protect dignity.
For elderly users, independence may look modest but it matters deeply.
Frailty-adjusted protocols allow older adults to move, stand, and live with confidence.
They honor both the body’s limits and the human spirit.
When care is designed with age in mind, prosthetics truly change lives.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body