
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


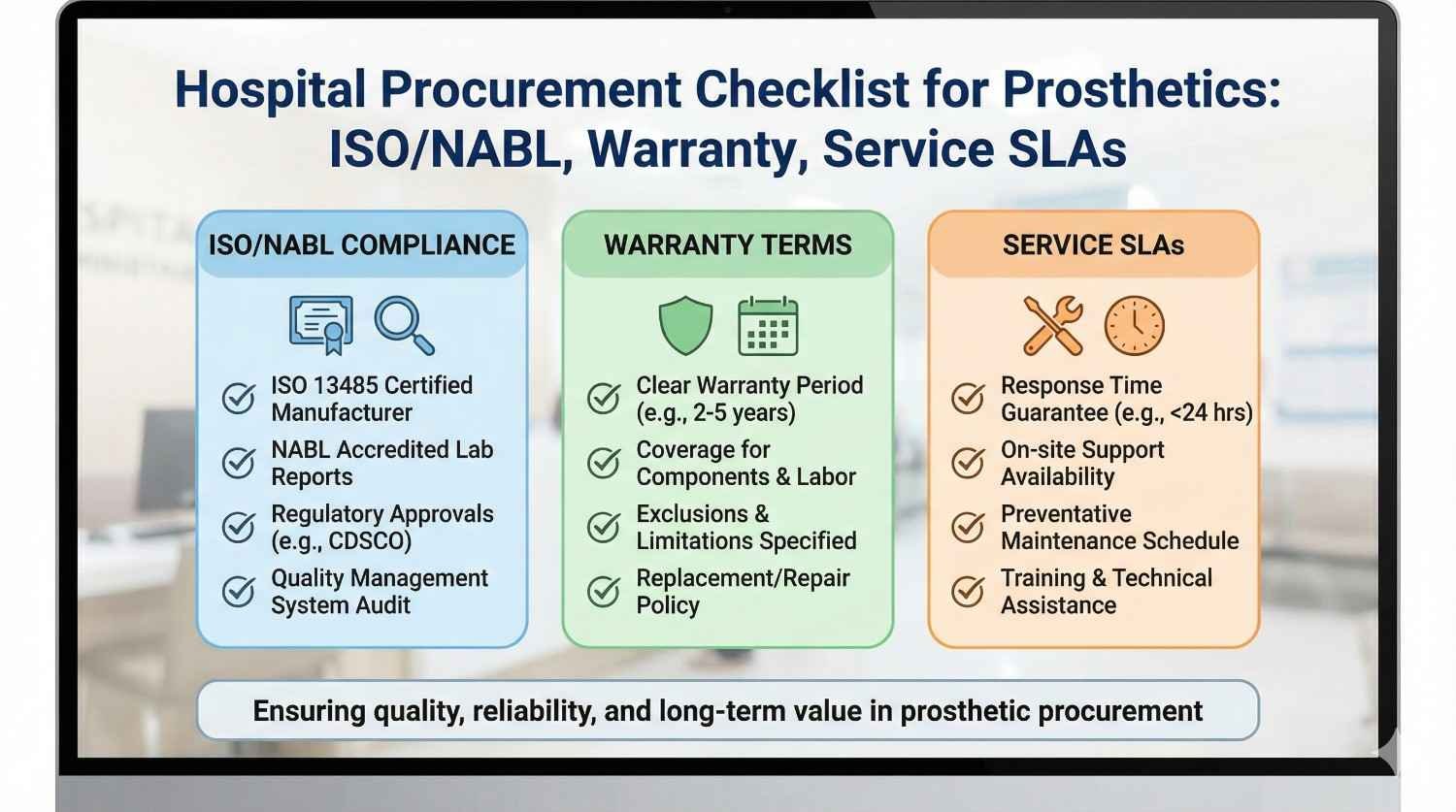
Hospital procurement teams carry a quiet but heavy responsibility. The prosthetic you approve today will shape a patient’s safety, comfort, and independence for years. Yet procurement decisions are often rushed, price-led, or based on incomplete checklists. This guide is written to change that. In simple words, it walks hospitals through what truly matters when procuring prosthetics in India—certifications, quality systems, warranties, service commitments, and long-term accountability—so decisions are safe, defensible, and patient-first.
Most medical devices remain inside hospital walls.
Prosthetics leave the hospital and become part of a patient’s daily life.
This changes responsibility completely.
Failure happens at home, at work, or on the road, not in a ward.
Procurement must think beyond delivery.
Long-term use is the real test.
A prosthesis is never finished on the day it is issued.
Fit changes, usage increases, and problems appear over time.
Without service support, even a good product fails.
Procurement must evaluate the service system behind the device.
This makes vendor capability as important as hardware quality.
Ignoring this leads to repeat failures.
When a prosthesis fails, patients return to the hospital.
Complaints, audits, and legal questions often follow.
Procurement decisions are reviewed closely in such cases.
Documentation and due diligence become critical.
A strong checklist protects the hospital.
It also protects patients.

ISO certification shows that a vendor follows a documented quality system.
It does not mean the product is perfect, but that processes are controlled.
For hospitals, this reduces variability risk.
It ensures repeatability and traceability.
ISO matters most when issues arise.
It shows systems exist to correct them.
ISO 13485 is specific to medical devices.
It covers design, manufacturing, and post-market processes.
For prosthetics, this certification is critical.
It shows the vendor understands medical risk management.
Hospitals should prefer vendors with ISO 13485.
It aligns with global best practice.
Some vendors show ISO certificates without scope clarity.
The certificate may not cover prosthetics.
Procurement teams should verify scope and validity.
A quick check prevents future trouble.
Certificates should be current and verifiable.
Old or vague documents are a warning sign.
NABL accreditation applies to testing and calibration labs.
It becomes relevant when mechanical or electrical testing is involved.
For bionic or powered prosthetics, testing credibility matters.
It supports safety and performance claims.
Hospitals should ask where testing is done.
Accredited labs add confidence.
Some vendors test in-house.
Others rely on external labs.
In-house testing is acceptable if systems are strong.
Third-party NABL labs add independent validation.
Procurement should understand both models.
Transparency is more important than location.
Test reports should be readable and relevant.
Generic reports add little value.
Hospitals should look for test purpose and limits.
Reports must link to real-world use.
Asking basic questions reveals quality.
Good vendors explain clearly.
A prosthesis may pass all lab tests and still fail users.
Daily life is harsher than controlled environments.
Hospitals should ask for field performance data.
This shows how devices behave in real conditions.
Clinical use history matters.
It reduces uncertainty.
Hospitals do not need academic trials for every device.
But usage data, case summaries, and outcomes help.
Evidence should reflect Indian conditions.
Climate, terrain, and user activity matter.
Local data is more useful than foreign brochures.
Context matters.
Marketing language often exaggerates capability.
Procurement should ask for examples, not promises.
A simple question like “where is this used” reveals much.
Real answers build trust.
Vendors who avoid specifics raise concern.
Evidence should speak.

A long warranty sounds attractive.
But coverage details matter more than duration.
Some warranties exclude key components.
Others limit usage conditions.
Hospitals must read what is actually covered.
Fine print decides value.
Warranty should clearly state parts and labor inclusion.
Ambiguity causes disputes.
Response timelines should be written, not implied.
Delays hurt patients and hospitals.
Clear terms reduce friction.
They protect all sides.
Liners, gloves, and cosmetic covers wear out.
Most warranties exclude them.
Hospitals should understand these exclusions.
Patients should be informed early.
Transparency prevents complaints later.
Expectation setting is part of care.
Service delays directly affect mobility and dignity.
A broken prosthesis is an emergency for the user.
Hospitals must ensure service SLAs are realistic.
Paper promises without capacity are risky.
SLAs show vendor seriousness.
They separate partners from sellers.
Some SLAs mention response but not resolution.
This creates false comfort.
Hospitals should insist on both.
Response without fix is not enough.
Clear escalation paths should exist.
This prevents endless waiting.
Remote support can solve many issues quickly.
On-site service is still essential for some cases.
Procurement should understand the service mix.
Coverage geography matters.
Vendors should explain how they support remote areas.
Silence here is a risk.
Prosthetics need parts over time.
Batteries, sensors, and joints may fail.
Hospitals should ask about parts availability period.
Support should extend for years, not months.
Lifecycle clarity protects patients.
It also protects hospital reputation.
Technology evolves quickly.
Old models may be discontinued.
Procurement should ask how vendors handle this.
Upgrade paths matter.
A clear obsolescence policy shows maturity.
It prevents stranded users.
Imported parts increase downtime.
Customs delays add uncertainty.
Vendors with local stocking respond faster.
This matters in emergencies.
Hospitals should factor this into evaluation.
Speed saves dignity.
A prosthesis is only as good as its training.
Poor training leads to abandonment.
Hospitals should ensure training is included.
It should not be optional.
Training scope and duration should be defined.
Vagueness leads to shortcuts.
Users change jobs and lifestyles.
Training needs evolve.
Procurement should check if refresher support exists.
This improves long-term outcomes.
Vendors who invest in training reduce failures.
It is a strong quality signal.
Clinicians and therapists need familiarity too.
This supports better follow-up.
Vendor-led staff training builds capability.
It strengthens partnership.
Hospitals should value this support.
It multiplies impact.
When issues arise, documents tell the story.
Missing records create risk.
Hospitals should demand clear documentation.
Device IDs, service logs, and warranty records matter.
Traceability is a safety net.
It supports audits and investigations.
Each prosthesis should be identifiable.
Serial numbers and batch details help.
Hospitals should integrate this into records.
This avoids confusion later.
Good vendors make this easy.
Poor ones resist.
Every service action should be logged.
This builds a history.
Hospitals should have access to these logs.
Transparency builds trust.
Logs also improve care quality.
Patterns emerge over time.
Many hospitals still evaluate prosthetic vendors using simple price tables.
While price matters, this method ignores the long-term cost of failures, rework, and patient dissatisfaction.
A stronger framework looks at total ownership cost.
This includes service load, replacement rates, training effort, and complaint handling.
Descriptive evaluation allows hospitals to defend decisions later.
It shows that value, not just price, drove selection.
Not all prosthetic components carry the same risk.
A failure in a powered hand or knee has higher impact than a cosmetic cover.
Procurement frameworks should assign higher weight to high-risk items.
This ensures quality and service depth are prioritized where consequences are serious.
Hospitals that apply risk-based weighting reduce adverse events.
They also reduce escalation to leadership.
Clinician input is essential but must be structured.
Unstructured opinions can introduce bias.
Hospitals should ask clinicians to score defined parameters.
Comfort, reliability, and ease of service are valid inputs.
This keeps evaluation balanced.
It respects expertise without personal preference dominating.
Hospitals often invite bids before verifying capability.
This leads to wasted time and weak options.
Pre-qualification should confirm certifications, service presence, and product maturity.
Only capable vendors should reach the price stage.
This saves effort later.
It also improves tender quality.
Strong pre-qualification protects procurement credibility.
It shows seriousness.
Certificates, test reports, and service commitments must be verified.
Photocopies and self-declarations are not enough.
Hospitals should insist on verifiable documents.
Online checks are quick and effective.
Verification reduces legal exposure.
It also discourages misrepresentation.
When possible, hospitals should visit vendor facilities.
Seeing manufacturing or service centers reveals much.
Cleanliness, process flow, and staff competence are visible signs.
They cannot be faked easily.
Site visits build confidence.
They also strengthen future collaboration.

Full upfront payment increases risk.
Hospitals lose leverage once payment is released.
Commercial terms should align payment with milestones.
Delivery, fitting stability, and early usage are reasonable points.
This encourages vendor follow-through.
It also aligns with patient outcomes.
Milestones should be realistic.
Fairness sustains partnerships.
Penalties should exist but be proportionate.
They should address repeated or serious failures.
Hospitals must avoid vague penalty language.
Clarity prevents disputes.
Penalties are not about punishment.
They are about accountability.
When defined well, they are rarely used.
Their presence drives discipline.
No partnership lasts forever.
Contracts should define how issues escalate.
Clear escalation paths avoid emotional conflict.
They keep resolution professional.
Termination clauses protect hospitals if risks persist.
They should be fair and structured.
Knowing there is an exit builds confidence.
It enables commitment.
Relying on a single vendor increases vulnerability.
Service disruptions or quality issues can halt care.
Some hospitals approve two vendors per category.
This balances continuity with competition.
Dual sourcing reduces dependency risk.
It also improves negotiation strength.
However, volume should not be spread too thin.
Balance is key.
Before large purchases, hospitals may run pilots.
Limited deployment reveals real-world issues.
Pilots test service SLAs under pressure.
They expose training and support gaps.
This reduces surprises during scale-up.
Learning happens early.
Pilots protect patients and budgets.
They are worth the time.
Procurement should not end at contract signing.
Performance must be reviewed regularly.
Service logs, complaints, and outcomes provide insight.
Trends matter more than single incidents.
Regular reviews encourage improvement.
They keep vendors engaged.
This approach turns procurement into governance.
It elevates its role.
Hospitals pursuing NABH accreditation face strict audit scrutiny.
Prosthetic procurement decisions are reviewed during audits.
Clear documentation, traceability, and vendor control help.
They show system maturity.
Procurement checklists should align with NABH standards.
This reduces audit stress.
Preparation avoids last-minute fixes.
It builds confidence.
When adverse events occur, procurement records are examined.
Incomplete due diligence increases liability.
Hospitals must be able to show why a vendor was chosen.
Evidence of evaluation protects decision-makers.
Clear contracts and records support incident response.
They reduce blame and confusion.
Preparedness is protection.
It matters deeply.
Hospitals are judged by outcomes, not tenders.
Poor prosthetic experiences harm reputation.
Strong procurement prevents these issues quietly.
It is invisible when done right.
Patients remember reliability.
Trust builds through consistency.
Procurement shapes this silently.
Its impact is profound.
At RoboBionics, compliance is not an afterthought.
Our products and processes are designed to meet hospital expectations.
Quality systems, documentation, and traceability are integral.
This supports procurement and audits.
We believe compliance enables innovation.
It does not restrict it.
Hospitals value predictability.
We deliver that.
We understand that service defines prosthetic success.
Our service SLAs are designed around patient urgency.
Local support, remote triage, and rapid resolution are prioritized.
Downtime is treated seriously.
This approach reduces hospital burden.
It improves user trust.
Partnership, not transactions, guide us.
That is our commitment.
We engage procurement teams openly.
Questions are welcomed, not avoided.
Documentation, site visits, and data sharing are part of our process.
Transparency builds confidence.
We see procurement as a clinical ally.
Not a hurdle.
This alignment improves outcomes for all.
Patients benefit most.

Hospitals are moving away from lowest-cost thinking.
Value and accountability are gaining importance.
Prosthetic procurement is at the center of this shift.
Outcomes are visible and personal.
Hospitals that adapt early lead the market.
They attract trust.
Procurement teams become strategic.
Their role expands.
Future procurement will link outcomes with vendor evaluation.
Service quality and patient usage will matter more.
Hospitals should begin collecting basic outcome data now.
This prepares them for future models.
Procurement and clinical teams must collaborate.
Silos weaken systems.
Integration strengthens decisions.
It improves care.
The future belongs to stable ecosystems, not rotating vendors.
Trust and performance compound over time.
Hospitals should invest in relationships that deliver.
Short-term savings rarely last.
A strong ecosystem reduces risk.
It improves resilience.
Procurement leadership defines this future.
Its choices matter.
Every procurement checklist should begin with one clear question: will this prosthesis remain safe and usable for the patient over time.
Price, brand, and delivery speed only matter after this question is answered with confidence.
Hospitals should ensure that safety thinking runs through every checkpoint.
From certification to service response, each item must support long-term use.
This mindset changes how checklists are applied.
They become tools for protection, not paperwork.
Hospitals should first confirm that the vendor operates under a valid quality management system relevant to medical devices.
ISO 13485 certification, with a clear scope that includes prosthetics, should be treated as essential, not optional.
Certification validity must be verified and current.
Expired or unclear certificates should pause procurement, not be explained away.
For powered or advanced prosthetics, testing credibility must be reviewed.
Hospitals should know where testing is done and whether NABL-accredited labs are involved.
These checks create a compliance baseline.
Without them, all other evaluation loses strength.
A prosthesis should not be treated as experimental equipment.
Hospitals should ask how long the product has been in regular clinical use.
Field usage data, even in simple form, adds confidence.
It shows how the device behaves outside brochures.
Hospitals should prefer products already proven in Indian conditions.
Climate, dust, and daily wear patterns matter deeply.
Maturity reduces risk.
It protects both patients and institutions.
Warranty terms must be read as operational documents, not marketing promises.
Hospitals should confirm what is covered, what is excluded, and how claims are handled.
Service SLAs should clearly define response time and resolution time.
A quick call-back without a fix is not real support.
Geographic service coverage must be realistic.
Hospitals should understand how remote or semi-urban patients will be supported.
Clear service assurance reduces future conflict.
It builds trust with users.
Procurement should always ask how long spare parts will be available.
Short-term support creates long-term problems.
Hospitals must understand the vendor’s policy on model discontinuation and upgrades.
Patients should not be stranded by product changes.
Local stocking of critical parts is a strong advantage.
It reduces downtime and stress during failures.
Lifecycle clarity is patient protection.
It also shields hospital reputation.
Initial user training must be included and clearly defined.
A prosthesis without proper training is incomplete care.
Hospitals should also check whether refresher training is available.
User needs evolve over time.
Support for hospital clinicians and therapists matters.
Vendor-led training improves follow-up quality.
Training commitments show seriousness.
They reduce abandonment risk.
Each prosthesis should be traceable to the vendor, batch, and service history.
This is essential for audits and incident reviews.
Hospitals should ensure that service actions are logged and accessible.
Transparency protects all parties.
Good documentation simplifies NABH audits and legal reviews.
It reduces stress during scrutiny.
Traceability is not bureaucracy.
It is safety infrastructure.
When vendors give unclear answers about service timelines or escalation, risk is high.
Strong vendors explain service clearly and confidently.
Evasion or overconfidence without detail should be treated cautiously.
Silence often hides weakness.
Hospitals should insist on written clarity.
Verbal assurances fade quickly.
Service gaps surface later.
Early caution prevents crisis.
Large discounts can signal pressure to close sales.
They may also signal compromises elsewhere.
Hospitals should ask what enables the discount.
Quality, service, or support should not be reduced.
Total value matters more than unit price.
Cheap failures are expensive.
Price should be one factor, not the driver.
Balance protects outcomes.
Vendors who avoid site visits or documentation checks raise concern.
Transparency is a sign of maturity.
Hospitals should be wary of excuses.
Serious partners welcome scrutiny.
Openness builds trust early.
Resistance erodes it.
Procurement should not feel rushed.
Time spent here saves years later.

Procurement choices signal what the hospital values.
Staff notice which vendors are approved and why.
When quality and service are prioritized, care culture strengthens.
Shortcuts become less acceptable.
This influence is subtle but strong.
It shapes behavior over time.
Procurement is leadership.
Its impact extends beyond contracts.
Clinicians perform better when tools are reliable.
Frequent prosthetic issues drain morale.
Strong procurement reduces daily friction.
It allows clinicians to focus on care.
This support is often invisible but deeply felt.
It improves retention and satisfaction.
Reliable systems build confidence.
Confidence improves outcomes.
Patients remember prosthetic success or failure vividly.
Hospitals are judged by these experiences.
Strong procurement prevents negative stories.
It builds positive word-of-mouth slowly.
Reputation grows through consistency.
Procurement decisions enable this.
Quiet success is the goal.
It is achieved through discipline.
At RoboBionics, we work closely with hospital procurement and clinical teams to align with these expectations.
Our approach is built around compliance, transparency, and long-term support.
We invest in quality systems, local manufacturing, and service infrastructure because we know hospitals depend on reliability.
Our documentation, training support, and service SLAs are designed to reduce hospital burden.
We engage procurement teams openly, welcome audits, and believe that clear answers build lasting trust.
Our focus is not just delivery, but sustained patient use and confidence.
For us, procurement success is measured by outcomes, not invoices.
That belief guides how we partner with hospitals across India.
Prosthetic procurement is not a routine purchase.
It is a long-term commitment to patient mobility, dignity, and safety.
Strong checklists protect hospitals legally, clinically, and reputationally.
They turn procurement from a risk point into a strength.
Hospitals that invest time in thoughtful procurement face fewer crises later.
They gain predictability, trust, and respect.
In an era of rising scrutiny and patient awareness, this discipline matters more than ever.
Procurement decisions today shape patient lives tomorrow.
Choosing well is not about complexity.
It is about asking the right questions and insisting on clear answers.
Many hospitals treat procurement checklists as one-time gatekeepers.
Once a vendor is approved, the checklist is forgotten.
In prosthetics, this approach creates blind spots.
Products, people, and service capacity change over time.
Hospitals should convert the checklist into a living system.
Regular reviews keep standards active.
Annual or biannual reassessment is enough.
Consistency matters more than frequency.
Procurement teams rarely hear day-to-day clinical pain points.
This gap weakens decision-making.
Simple feedback loops can fix this.
Quarterly inputs from prosthetists, therapists, and rehab teams add real value.
Patterns of repair, delay, or dissatisfaction should inform vendor scores.
This keeps procurement grounded in reality.
When clinical voices are heard, trust improves.
Systems become smarter, not heavier.
Over time, hospitals build powerful internal data.
Service delays, part failures, and training gaps tell clear stories.
Procurement teams should capture and review these signals.
They predict future problems early.
This turns procurement into risk prevention.
It reduces reactive decision-making.
Data-driven governance builds confidence at leadership level.
It strengthens institutional resilience.
Audits are stressful only when preparation is weak.
Strong procurement systems make audits routine.
Clear vendor files, updated certificates, and service records should be easily accessible.
No scrambling should be required.
Hospitals that maintain audit-ready procurement sleep better.
They respond calmly under scrutiny.
Audit readiness is not extra work.
It is organized work.
When prosthetic issues escalate, procurement decisions come under review.
Hospitals must be able to explain why a vendor was chosen.
A well-documented checklist answers this clearly.
It shows due diligence and reasonable care.
This protects the hospital and its staff.
It also supports fair resolution.
Preparedness reduces blame.
It encourages constructive action.
In legal reviews, intent and process matter.
Hospitals must show that choices were informed and responsible.
Procurement checklists provide this evidence.
They show that decisions followed defined criteria.
This reduces personal risk for committees.
It protects institutional reputation.
Structure is a shield.
It matters more than opinions.
Prosthetics combine medical risk, long-term service, and patient behavior.
This makes them different from most medical purchases.
Procurement teams need basic prosthetic literacy.
Understanding lifecycle, wear, and follow-up changes evaluation quality.
Even short orientation sessions help.
They build confidence and accuracy.
Knowledge reduces dependency on vendor claims.
It empowers teams.
Strong hospitals do not isolate procurement.
They involve clinical, rehab, and quality teams.
Cross-functional committees reduce blind spots.
They balance cost, care, and compliance.
These committees do not need to meet often.
Even periodic reviews add value.
Shared ownership improves decisions.
It also spreads accountability.
Procurement decisions affect real lives.
Teams should be reminded of this.
Ethical framing improves judgment.
It shifts focus from speed to safety.
Hospitals that reinforce patient-first procurement build strong culture.
Culture outlasts policies.
This mindset protects everyone.
It defines institutional character.

Patients today ask more questions.
They research devices and expect explanations.
Hospitals will face greater scrutiny on choices.
Procurement transparency will matter.
Strong systems prepare hospitals for this future.
Weak ones will struggle.
Accountability is rising.
Preparation is the only answer.
Procurement will increasingly link with outcomes.
Service quality and patient use will influence vendor standing.
Hospitals should begin aligning procurement with outcome thinking.
This transition takes time.
Early movers gain confidence and control.
Late movers face pressure.
Value-based care is coming.
Procurement must be ready.
The future favors stable partnerships.
Constant vendor rotation increases risk.
Hospitals that build trusted ecosystems gain predictability.
Quality improves steadily.
Procurement leaders shape this future.
Their choices compound over years.
Stability benefits patients most.
That is the true goal.
Hospital prosthetic procurement is not a routine operational task.
It is a long-term promise to patients who depend on mobility for dignity and livelihood.
A strong procurement checklist built around ISO, NABL awareness, warranty depth, and service SLAs protects that promise.
It safeguards hospitals clinically, legally, and reputationally.
When procurement is done with care and clarity, problems reduce quietly.
Clinicians feel supported, patients feel secure, and leadership feels confident.
At RoboBionics, we believe hospitals deserve partners who respect this responsibility.
We design our systems, services, and documentation to support safe, transparent procurement.
Choosing the right prosthetic partner is not about complexity.
It is about asking clear questions and expecting clear answers.
That discipline is what turns procurement into a pillar of patient trust.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body