
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation



Pain is often the first and biggest wall between an amputee and early prosthetic use. As medical doctors, you see this every day. A well-done surgery can still be followed by pain that delays fitting, slows rehab, and affects long-term outcomes. When pain is not handled early and in the right way, patients lose confidence, motivation, and valuable recovery time.
Early prosthetic use is not just about giving a device quickly. It depends on how well pain is managed from day one. When pain pathways are planned properly, patients heal faster, adapt sooner, and accept their prosthesis with far less fear and resistance. This directly improves function, mental health, and overall quality of life.
This article is written for MDs who want practical, real-world pathways to manage pain in a way that supports early prosthetic fitting. No heavy theory. No complex terms. Just clear, usable guidance based on what works on the ground in India and similar settings.
Pain after amputation is not only discomfort. It directly affects wound healing, limb shaping, muscle activation, and patient trust. When pain is high, patients avoid movement, delay sitting balance, and resist early loading. This slows every next step in rehabilitation.
Many patients also start linking pain with failure. They begin to believe that prosthetic use will always hurt. Once this belief forms, it becomes much harder to reverse, even when tissues heal well.
The first few weeks after surgery decide how the brain remembers the limb. If pain is constant and unmanaged, the nervous system stays alert and overprotective. This increases the risk of chronic pain and phantom limb pain later.
On the other hand, when pain is controlled early, patients move sooner, sleep better, and engage more. This creates a positive loop that supports faster prosthetic readiness.
MDs are often the first and most trusted guides for patients. The way pain is explained, treated, and followed up sets the tone for recovery. A clear pain plan builds confidence and prepares the patient mentally for early prosthetic use.
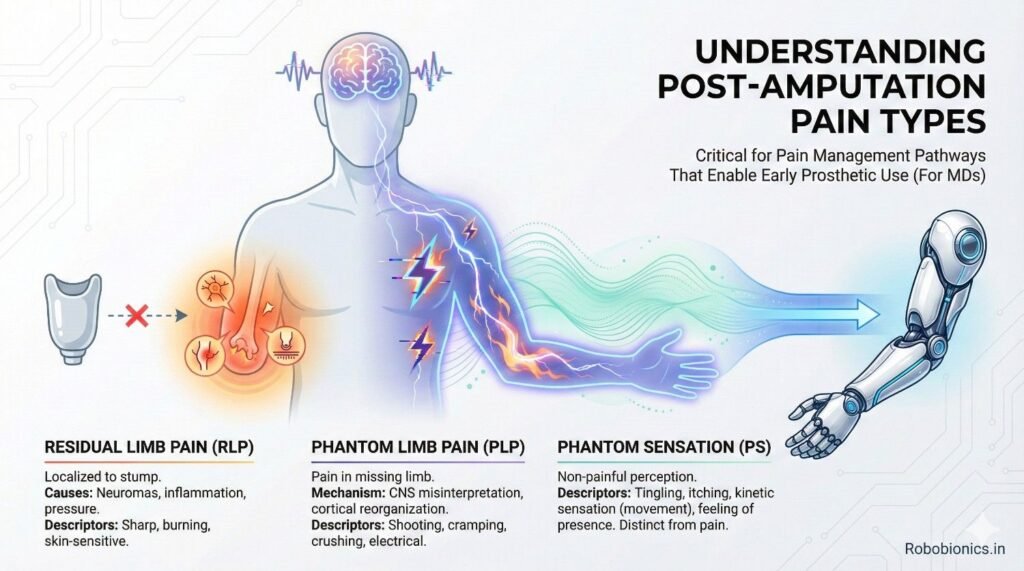
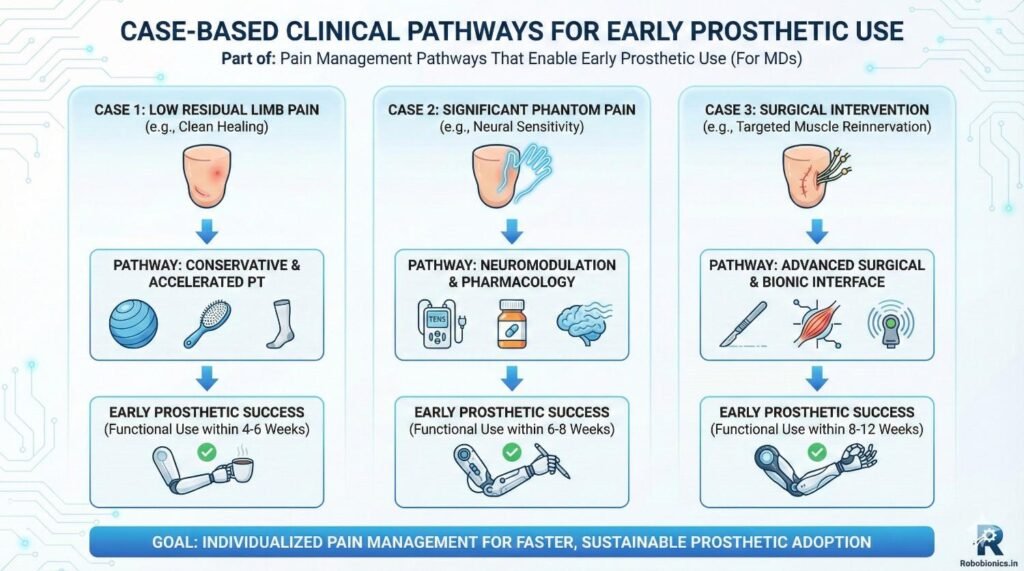
This is expected pain from tissue cutting, muscle handling, and bone work. It is strongest in the first days and should reduce steadily. If it does not reduce, it often signals infection, poor wound care, or nerve irritation.
Clear differentiation between normal healing pain and warning pain helps patients stay calm and compliant.
Residual limb pain comes from skin, muscle, bone, or nerves in the stump. Poor limb positioning, tight dressings, or uneven pressure can increase it. This pain directly affects tolerance to temporary sockets or early prosthetic trials.
Early attention to stump shape, skin health, and pressure points can reduce this pain significantly.
Phantom pain is real pain felt in the missing limb. It is driven by brain and nerve changes, not imagination. Ignoring or dismissing it often makes it worse.
Addressing phantom pain early helps patients accept their body changes and reduces fear around prosthetic use.
This pain feels sharp, burning, or electric. It often comes from nerve injury or neuroma formation. If not treated early, it becomes chronic and very hard to manage.
MDs play a key role in early identification and referral when neuropathic patterns appear.
Pain control should not be reactive. It must be planned before surgery and continued through rehab. A clear pathway aligns surgeons, physicians, therapists, and prosthetists.
When everyone works from the same plan, patients receive consistent messages and better care.
Early, steady pain control is better than strong medicines given late. Large pain spikes teach the nervous system to stay alert. Smaller, controlled pain levels allow safer movement and early loading.
This approach supports faster limb conditioning and prosthetic readiness.
Using only medicines rarely works well. Combining medicines with positioning, therapy, education, and early limb use gives better results. Each method supports the other and reduces dependence on any single tool.
Pain medicines should be chosen with function in mind. The goal is not zero pain at rest, but tolerable pain during movement. This allows early sitting, standing, and limb handling.
Over-sedation delays rehab and reduces patient engagement.
Clear timelines help patients understand that medicines are support tools, not lifelong needs. This reduces fear and misuse. Regular review allows safe tapering as healing improves.
When nerve pain signs appear, early treatment prevents long-term problems. Delay allows nerve pathways to harden and become resistant to treatment.
Simple explanations help patients accept nerve-focused treatments early.
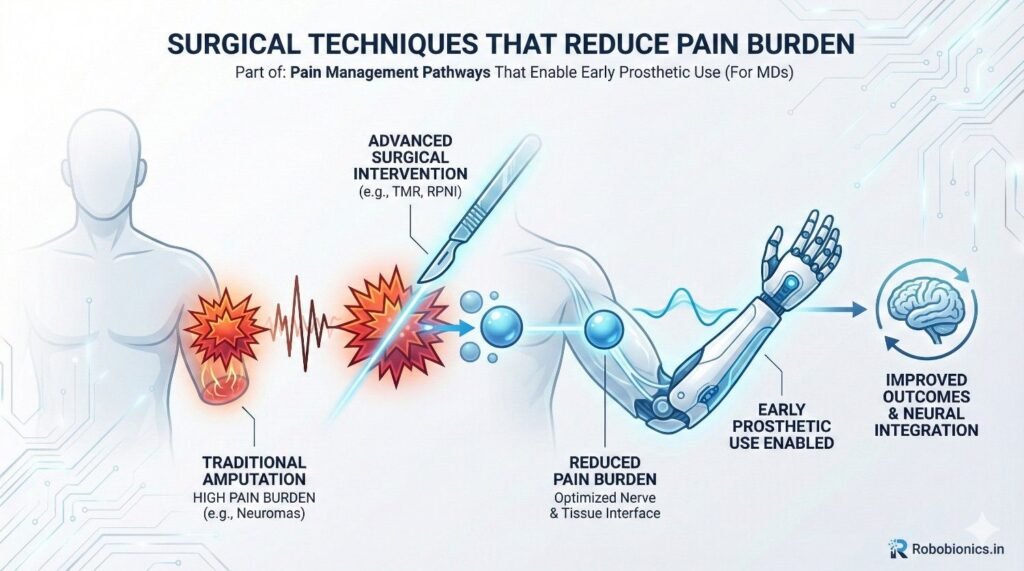
Clean surgical planes and careful nerve handling reduce later pain. Even small improvements during surgery can lead to big gains during rehab.
Good surgical notes also help rehab teams understand risk areas.
Addressing nerves during amputation reduces neuroma risk. This directly lowers residual limb pain and improves prosthetic comfort.
Early communication between surgeon and rehab team improves follow-up care.
A well-shaped limb reduces pressure pain later. This allows earlier socket trials and reduces repeated fitting delays.
Patients benefit when surgical goals include prosthetic readiness from the start.
Gentle, guided movement reduces swelling and stiffness. This lowers pain naturally and builds trust in the limb. Avoiding movement often increases pain over time.
Early physiotherapy should focus on safe, pain-aware motion.
Simple touch, textures, and pressure help the brain accept the limb. This reduces fear and pain during socket contact.
MD encouragement makes patients more willing to try these steps.
Correct limb positioning prevents joint stiffness and skin pain. Small daily habits make a large difference over weeks.
Clear instructions reduce confusion and anxiety.
Fear of pain often increases pain itself. Patients who expect pain tense their muscles and avoid movement. This worsens stiffness and discomfort.
Clear reassurance from MDs reduces this cycle.
Explaining what pain is normal and what is not builds trust. Patients feel safer when they know what to expect.
This trust improves cooperation with early prosthetic steps.
Loss of a limb affects self-image deeply. Emotional pain can delay prosthetic acceptance even when physical pain is controlled.
Acknowledging this openly improves outcomes.
Prosthetists can guide stump care even before fitting. Their input helps reduce pressure pain later.
Early referrals shorten the overall rehab timeline.
Early devices help patients learn pressure tolerance. Pain feedback guides socket adjustments and limb conditioning.
This reduces fear of the final prosthesis.
When MDs, therapists, and prosthetists use the same pain language, patients feel supported. Mixed messages increase anxiety and pain focus.
Consistency improves confidence and outcomes.
Patients should know that some pain is part of healing. At the same time, they should know that pain can be controlled and will reduce.
Balanced messaging prevents disappointment and fear.
Explaining how pain management leads to faster independence motivates patients. They become active partners in their care.
This mindset supports early prosthetic use.
Families influence pain behavior strongly. Educating them reduces overprotection and fear-based advice.
This creates a better recovery environment.
Regional pain control methods play a strong role in allowing early movement without overwhelming discomfort. When pain relief is focused around the surgical area instead of the whole body, patients remain alert, cooperative, and confident during early rehabilitation. This clarity helps them participate actively in stump care, positioning, and gentle loading, which are all required for early prosthetic planning. From a functional point of view, regional approaches reduce guarding behavior, where patients unconsciously tighten muscles due to fear of pain, leading to stiffness and delayed healing.
For MDs, the key is to align pain control with rehabilitation timelines. Pain relief should last long enough to allow early sitting, transfers, and limb handling, but not so long that patients disconnect from their body signals. When patients can feel mild, safe sensations without sharp pain, they begin trusting their limb again. This trust is essential before introducing any prosthetic contact.
Complete numbness may feel ideal in the short term, but it can delay adaptation. Sensory input helps the brain reorganize after limb loss. When pain control removes all sensation, patients often struggle later when sensation returns suddenly during prosthetic use. A balanced approach allows safe sensory feedback while avoiding severe pain spikes.
Explaining this clearly to patients builds cooperation. When patients understand that some awareness helps healing, they are less anxious and more willing to engage in therapy. This mindset prepares them mentally for socket contact and pressure later.
Numeric pain scores are useful, but patterns matter more. Pain that reduces with movement is different from pain that increases with loading. Pain that improves daily is different from pain that stays fixed. MDs who track these patterns can intervene earlier and guide rehab teams more effectively.
This approach also helps in early identification of neuropathic pain, infection, or poor limb mechanics, all of which can delay prosthetic use if missed.
Phantom limb pain often begins in the early post-operative phase, even if patients do not describe it clearly. Subtle signs like strange sensations, tingling, or discomfort in the missing limb should not be ignored. Early acknowledgment reduces fear and prevents patients from thinking something is wrong or abnormal.
When MDs normalize these sensations and explain the brain’s role, patients feel reassured. This reduces stress, which itself lowers pain intensity.
Simple sensory exercises help the brain adjust to limb loss. Techniques like gentle touch, vibration, and visual feedback support brain re-mapping. These methods are low-cost, easy to explain, and effective when started early.
From a clinical perspective, early sensory re-education reduces later phantom pain severity and improves acceptance of prosthetic sensation. Patients who understand their sensations are more open to advanced prosthetic features later.
Delayed prosthetic exposure increases phantom pain risk. When the brain has no physical reference for the missing limb, it fills the gap with pain signals. Early temporary prosthetic use gives the brain a new reference point.
Even light socket contact without full weight-bearing can reduce phantom sensations and improve emotional adjustment.
Most early prosthetic delays come from skin issues, not deep pain. Fragile skin, blisters, and minor wounds create fear and reduce wear time. Simple daily skin care routines prevent these issues.
MDs who emphasize skin inspection and hygiene early reduce complications later. Clear instructions and demonstrations improve patient compliance.
Swelling increases pressure pain and delays socket fitting. Consistent compression and proper positioning reduce edema and improve limb shape. This directly affects socket comfort and fitting speed.
Patients who understand the purpose of compression are more disciplined. This education saves weeks in the prosthetic timeline.
Gentle loading strengthens tissues and reduces deep residual limb pain over time. Avoiding all pressure often increases sensitivity. Gradual exposure builds tolerance and confidence.
MD reassurance helps patients overcome fear and engage in these steps safely.
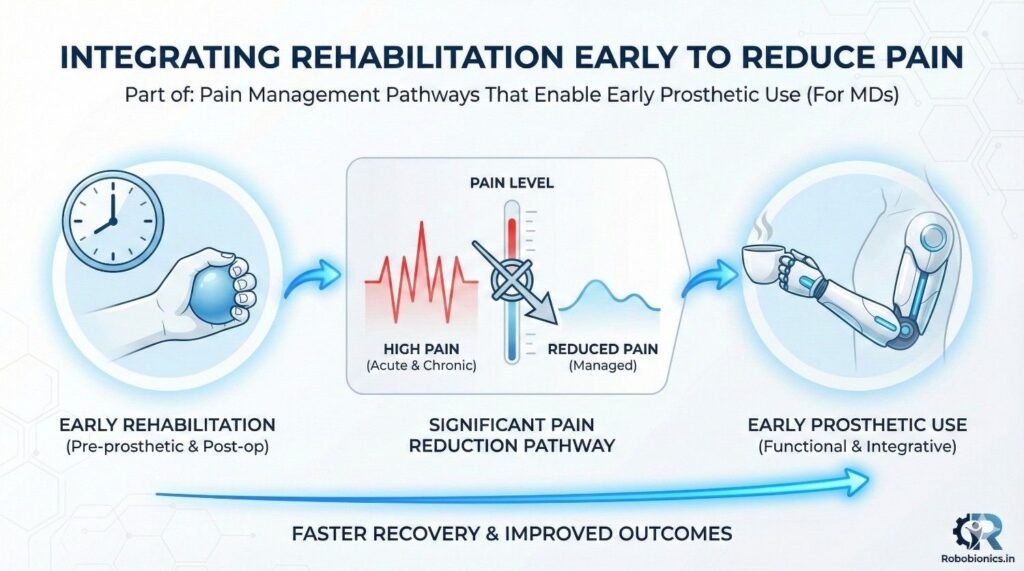
Waiting for pain to fully stop before starting rehab is a common mistake. Controlled movement actually reduces pain by improving circulation and reducing stiffness. Early rehab must be guided and pain-aware, not aggressive.
MDs who actively prescribe early rehab send a strong signal that movement is safe and necessary.
Targeted strengthening of the core and remaining limb reduces load on the residual limb. This lowers compensatory pain and fatigue. Balanced strength improves prosthetic outcomes later.
Clear communication between MDs and therapists ensures exercises match healing stages.
Back pain, shoulder pain, and joint pain often appear when mobility is limited. Early rehab prevents these issues, which otherwise delay prosthetic training.
Addressing the whole body reduces overall pain burden and improves readiness.
Stress, fear, and sadness increase pain sensitivity. Patients who feel heard and supported report lower pain even with similar physical findings. This is not imagined pain, but real nervous system response.
MDs have a unique role in shaping this emotional environment through words and behavior.
The words used to describe pain matter. Saying pain is expected and manageable reduces fear. Warning patients excessively about pain increases vigilance and discomfort.
Clear, calm explanations improve pain tolerance and cooperation.
Regular check-ins reassure patients that pain is monitored and temporary. This reduces anxiety-driven pain escalation.
Trust improves adherence to rehab and prosthetic plans.
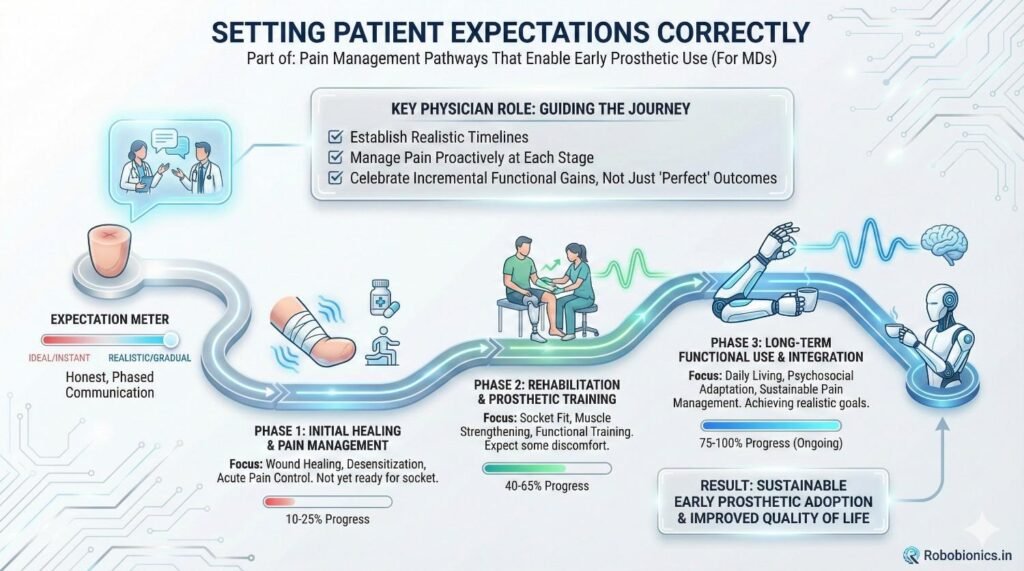
Patients benefit from knowing what comes next. Clear timelines for wound healing, limb shaping, and prosthetic trials reduce uncertainty. This clarity lowers stress and improves pain control.
MDs who set expectations early reduce dropouts and delays.
Pain management works best when teams communicate. Surgeons, physicians, therapists, and prosthetists must align goals and language. Mixed advice increases confusion and pain focus.
Simple shared protocols improve outcomes.
In India and similar settings, access and cost matter. Pain pathways must be practical and affordable. Simple methods, done consistently, often outperform complex plans that patients cannot follow.
MD leadership ensures realistic and effective care.
Temporary prostheses are not just placeholders. They teach pressure tolerance, balance, and confidence. Early exposure reduces fear of the final device.
Patients who experience early success report lower pain later.
Short, frequent sessions are better than long, painful ones. This approach trains both body and brain. MD reinforcement helps patients follow this plan.
Consistency matters more than intensity.
Pain feedback guides socket changes. Encouraging patients to report discomfort early prevents major issues later.
This proactive approach speeds up final fitting.
The ability to sit, stand, transfer, and tolerate socket contact matters more than a pain number. These milestones predict prosthetic success better than pain scores alone.
MDs should track these markers actively.
Confidence predicts usage. Patients who feel capable use their prosthesis more, even if some discomfort exists. Supporting confidence reduces perceived pain.
This is a key but often overlooked outcome.
Early pain control leads to early prosthetic use, which leads to better long-term independence. This reduces healthcare burden and improves quality of life.
MDs play a central role in this chain.
In younger traumatic amputees, pain is often mixed with fear and sudden loss of control. These patients may heal fast physically, but mentally they struggle with uncertainty. Pain feels sharper because the event was unexpected, and the body has not had time to adapt. In such cases, early reassurance and clear explanations reduce pain perception more than increasing medicines.
A structured pathway works best. From day one, pain is explained as a temporary phase with a clear end goal of prosthetic use. Early stump handling, visual exposure, and simple exercises reduce fear. When pain is framed as a step toward independence, patients engage more actively. Early temporary prosthetic trials, even for short standing sessions, reduce both pain and anxiety.
These patients often have lower pain intensity but longer pain duration. Poor circulation, fragile skin, and slow healing create repeated setbacks. Pain here is often dull, persistent, and frustrating rather than sharp. The biggest risk is delay, not intensity.
For this group, consistency matters more than speed. Gentle pain control combined with strict skin care and edema management supports gradual progress. Early prosthetic planning must be realistic, with close monitoring. Clear communication prevents disappointment and dropout. When patients see steady improvement, pain feels more manageable and less threatening.
Older patients often underreport pain but show it through withdrawal and low participation. Sedation from pain medicines can worsen confusion and increase fall risk. Here, the goal is safe comfort, not aggressive pain elimination.
Simple routines, predictable schedules, and familiar caregivers reduce stress-related pain. Early seating balance, transfers, and light prosthetic exposure improve confidence. Pain reduces when patients feel stable and supported rather than rushed.
One of the most common mistakes is waiting for pain to fully stop before allowing movement. This often leads to stiffness, swelling, and increased sensitivity. By the time movement starts, pain is worse, not better.
Early, guided movement reduces pain naturally. MDs who delay rehab unintentionally increase long-term pain and prosthetic resistance.
Medicines without movement, education, and limb care rarely succeed. Patients become passive and fearful of activity. When medicines reduce pain but do not build confidence, prosthetic use remains delayed.
Balanced pathways that combine medicine with action produce better outcomes.
Minor skin pain or pressure discomfort often signals future problems. When ignored, these grow into wounds or chronic pain. Early attention saves weeks of delay later.
Encouraging patients to speak openly about pain builds trust and prevents complications.
Conflicting advice increases anxiety and pain focus. If one team encourages movement while another warns against it, patients choose avoidance. Clear, shared messaging reduces confusion and pain.
MDs often act as coordinators and must ensure alignment.
Pain planning should start before surgery whenever possible. Explaining expected pain, recovery stages, and prosthetic goals reduces shock later. Setting realistic timelines prepares patients mentally.
Early involvement of rehab teams improves continuity.
Pain control should allow alertness and basic movement. Limb positioning, gentle handling, and early education begin here. Monitoring pain patterns daily guides adjustments.
Clear documentation supports team coordination.
Movement, desensitization, and limb care become priorities. Pain should reduce steadily. Any increase must be investigated early.
Encouraging independence builds confidence and lowers pain perception.
Residual limb tolerance, skin health, and confidence are key markers. Pain should be predictable and manageable. Addressing fears at this stage improves fitting success.
Early prosthetist involvement shortens timelines.
Not all pain is harmful. Stretching pain, pressure awareness, and mild soreness often signal adaptation. Sharp, worsening, or night pain may signal problems.
Teaching patients to understand this difference reduces fear and over-reporting.
Pain guides pacing. When used correctly, it prevents overloading without stopping progress. Flexible pathways respond to pain rather than rigid timelines.
MD judgment is central here.
Patients who understand their pain manage it better. They become partners, not passive recipients. This improves long-term prosthetic use.
Education is a powerful pain tool.
How patients treat their limb early affects long-term comfort. Gentle care, regular inspection, and gradual loading build durable tolerance.
Poor early habits lead to chronic sensitivity.
Prostheses are not pain-free at all times. Mild pressure and effort are normal. Preparing patients for this prevents disappointment and device rejection.
Honest conversations improve satisfaction.
When pain management is connected to work, family roles, and independence, patients stay motivated. Pain feels meaningful, not pointless.
This mindset improves adherence and outcomes.
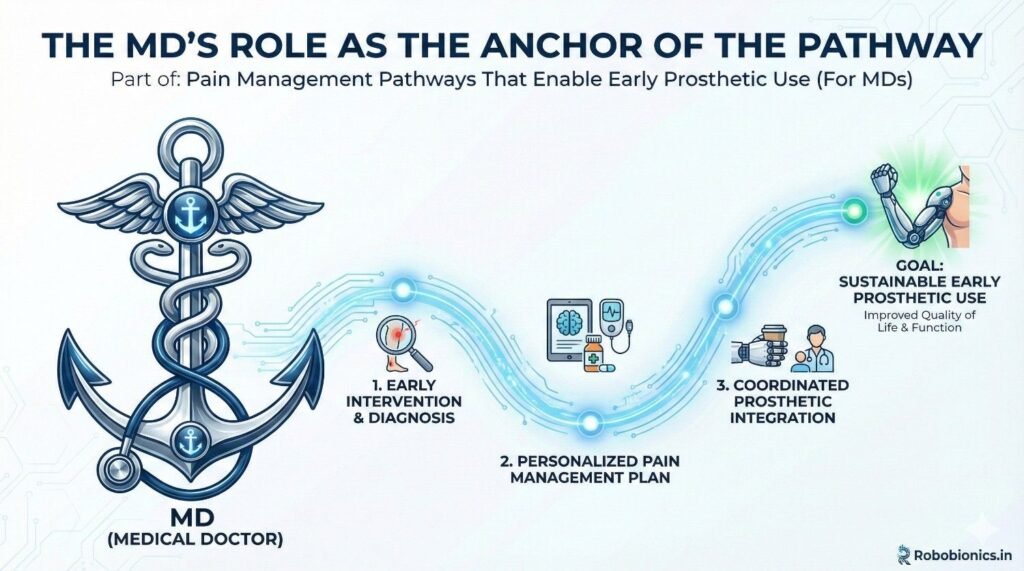
MDs influence patient belief systems. Calm confidence reduces fear-driven pain. Clear direction prevents confusion.
This leadership shapes the entire rehab journey.
When MDs actively support early prosthetic trials, teams align faster. Patients feel reassured that early use is safe and expected.
This reduces unnecessary delays.
Pain science and prosthetic care evolve. MDs who stay updated improve outcomes. Learning from prosthetists and therapists strengthens pathways.
Collaboration improves care quality.
Early control reduces long-term pain syndromes. This lowers future healthcare needs and improves quality of life.
Prevention is more effective than treatment.
Patients who start early use their prosthesis more consistently. Confidence replaces fear.
This leads to better functional outcomes.
Early prosthetic use supports return to work and social roles. Pain control plays a silent but powerful role in this success.
MDs contribute directly to this impact.
Even the best pain strategies fail when they depend only on individual effort. Sustainable success comes when hospitals and clinics build pain pathways into routine care. This means pain planning is not optional or doctor-dependent, but a standard part of amputation management. When systems support early pain control, outcomes become predictable and repeatable.
For MDs, this reduces decision fatigue and improves consistency. Patients receive similar guidance regardless of who is on duty. This consistency alone reduces anxiety-driven pain and builds trust in the system.
Protocols should guide, not restrict. A clear framework for pain control, early movement, stump care, and prosthetic referral helps teams act early. At the same time, MDs must retain flexibility to adjust based on patient response.
Well-designed pathways highlight red flags, expected milestones, and referral points. This structure prevents delays while respecting clinical nuance.
When teams understand that the end goal is prosthetic use, pain management changes naturally. Nurses handle limbs more confidently, therapists push movement safely, and patients sense a shared direction.
Regular team discussions and simple training sessions reinforce this mindset. Over time, early prosthetic readiness becomes the norm, not the exception.
Pain control should be planned from admission, not after surgery. Documenting expected pain phases, medicine plans, and rehab timelines prepares the entire team. This also helps during handovers and discharge planning.
Patients who leave the hospital with a clear pain and rehab plan are less likely to return with complications.
Waiting for full wound healing before prosthetic referral is outdated. Protocols should define clear triggers for early prosthetist involvement, such as stable wounds, controlled pain, and basic limb tolerance.
Early referrals shorten the total rehab journey and reduce patient frustration.
Clear notes on pain type, triggers, and response help downstream teams. This prevents repeated trial-and-error and builds on previous progress.
Good documentation is a silent but powerful tool for pain control.
Early prosthetic success depends on collaboration. Prosthetic partners must understand pain pathways and respect healing stages. Choosing partners who value communication and patient education improves outcomes.
Strong partnerships reduce blame-shifting and delays.
Case discussions between MDs, therapists, and prosthetists align goals early. These discussions prevent mismatched expectations and reduce patient confusion.
Even brief coordination meetings can save weeks later.
Pain feedback from prosthetic trials should return to the medical team. This loop allows early correction of surgical, rehab, or fitting issues.
Learning from each case strengthens the pathway over time.
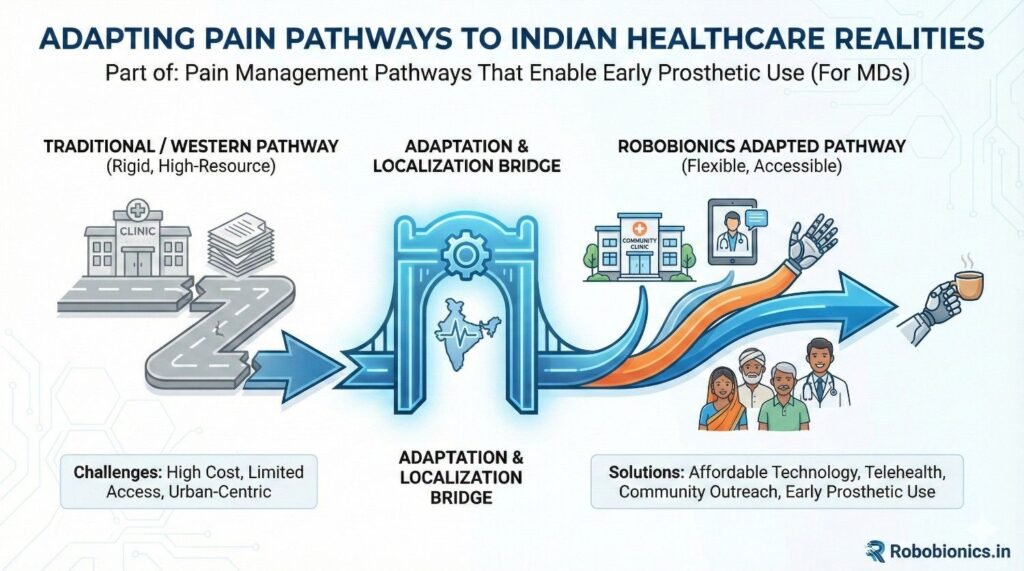
In resource-limited settings, expensive interventions are not always possible. Fortunately, many effective pain strategies are low-cost. Education, positioning, early movement, and timely reassurance cost little but deliver high impact.
MD leadership ensures smart use of available resources.
Many patients travel long distances and have limited follow-up access. Pain pathways must account for this reality. Clear home-care instructions, family education, and early prosthetic planning reduce dependence on frequent visits.
Simple written or visual guides improve adherence.
Pain expression varies widely. Some patients underreport pain, while others express it strongly. Understanding cultural context helps MDs interpret pain accurately.
Respectful listening builds trust and improves reporting accuracy.
Effective pain management is a continuous process that supports healing, movement, and confidence. Medicines are tools, not solutions. When pain control is aligned with function, early prosthetic use becomes achievable.
MDs who adopt this view see better outcomes consistently.
Prosthetic readiness is shaped in the first weeks after amputation. Delays during this phase are hard to reverse. Early planning, education, and exposure change the trajectory of recovery.
Every day matters in this window.
How pain is explained shapes how it is felt. Calm, confident communication reduces fear and improves tolerance. Patients remember reassurance long after medicines wear off.
MDs are powerful influencers of pain perception.
No single professional controls the outcome alone. When MDs lead collaborative care, pain pathways become stronger and more reliable. Shared goals reduce delays and frustration.
Team-based care is not optional in modern prosthetic rehabilitation.
Pain after amputation is unavoidable, but prolonged suffering and delayed prosthetic use are not. With structured, early, and human-centered pain pathways, patients can move faster from loss to independence. Early prosthetic use is not just a rehabilitation milestone. It is a signal that pain has been understood, respected, and guided in the right direction.
As medical doctors, your role sits at the center of this journey. When pain is managed with purpose, clarity, and compassion, prosthetic success follows naturally.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body