
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Upper-limb loss changes how a person eats, works, communicates, and takes care of daily life. For physicians, deciding when to prescribe an upper-limb prosthesis is a clinical responsibility that goes far beyond replacing a missing hand or arm. The timing, intent, and type of prescription can shape a patient’s recovery, confidence, and long-term independence.
This guide is written to help physicians make clear, practical decisions about upper-limb prosthetic prescription. It focuses on real clinical situations, simple reasoning, and patient-centered judgment, so prosthetic care becomes a natural and effective part of treatment.
An upper-limb prosthesis does not only replace a missing body part.
It supports daily actions like holding, lifting, stabilizing, and expressing.
These actions shape independence and self-worth.
Physicians should see upper-limb prosthetics as functional tools.
They reduce dependence on caregivers.
They also help patients return to social and work roles.
When prescribed with purpose, prosthetics become part of recovery.
They are not cosmetic add-ons.
They are clinical interventions.
Upper-limb prosthetics are used by choice, not necessity.
A person can walk without a hand prosthesis, but life becomes harder.
This makes acceptance and usefulness deeply personal.
Fine motor tasks, comfort, and learning effort matter more here.
If the device does not help daily life, it will not be worn.
Physicians must judge benefit carefully.
This is why indication clarity is critical.
Wrong timing or wrong intent leads to rejection.
Right decisions lead to long-term use.
Physicians often decide whether prosthetic care even begins.
Early referral shapes expectations and rehab planning.
Late referral often leads to missed opportunity.
Clear prescriptions guide prosthetists and therapists.
Vague or delayed decisions create confusion.
Good outcomes start with good medical judgment.
Physicians also help patients trust the process.
Their words carry weight early after limb loss.
That influence should be used wisely.
The patient must be medically stable before fitting.
Infection, unstable wounds, or uncontrolled pain must be addressed first.
Prosthetic fitting adds stress to healing tissue.
Surgical healing should be reliable, not just improving.
Scar condition and skin tolerance matter.
Rushing this step often causes failure.
Physicians should coordinate with surgeons closely.
Readiness is a shared decision.
Safety always comes first.
The length, shape, and sensitivity of the residual limb affect success.
Preserved joints increase control and comfort.
Painful scars or poor skin tolerance reduce use.
Range of motion at the shoulder and elbow is critical.
Stiffness limits function more than strength alone.
Early therapy prevents future limitations.
Physicians should assess movement actively.
Do not rely only on notes.
Functional exam gives better insight.
Upper-limb prostheses require learning and patience.
Patients must understand basic training steps.
They must also recognize discomfort and danger.
This does not require high education.
It requires awareness and engagement.
Many patients succeed with proper support.
Physicians should assess understanding gently.
Involve family when needed.
Support often determines success.
Upper-limb prosthetic use is driven by purpose.
Patients who see daily value adapt better.
Those without clear goals often abandon use.
Physicians should ask about daily tasks.
Eating, dressing, work, and hobbies matter.
These answers guide prescription intent.
Motivation can grow with education.
It should not be assumed or dismissed early.
Conversation shapes readiness.
Partial hand loss is often underestimated.
Even small losses affect grip and precision.
Indications arise when daily tasks become difficult.
Patients may struggle with writing, tools, or cooking.
Pain or overuse of the other hand is common.
Prosthetic support can restore balance.
Early prescription prevents poor compensation habits.
Simple devices often provide strong benefit.
Physicians should not delay referral.
Below-elbow loss has strong prosthetic potential.
Elbow movement allows good control.
This level often benefits most from prosthetic care.
Indications include difficulty with bimanual tasks.
Stabilizing objects and lifting become hard.
A prosthesis restores symmetry in function.
Physicians should consider early fitting.
Training success is usually higher.
Long-term use is more likely.
Above-elbow prosthetic prescription is more complex.
Control demands and energy use increase.
Training time is longer.
Indications depend on shoulder health and endurance.
Patients must be willing to train consistently.
Goals should be realistic and specific.
Some patients may start with simpler devices.
Others may prefer staged progression.
Physician guidance is key here.
These levels present major functional challenges.
Prosthetic use is demanding and highly individual.
Indications must be considered carefully.
Some patients benefit from stabilization or cosmetic support.
Others may focus on balance and appearance.
Functional goals may be limited.
Physicians should avoid assumptions.
Trial and patient preference matter greatly.
Support should remain ongoing.
Early discussion helps patients understand options.
Referral does not mean immediate fitting.
It means planning begins early.
Early education reduces fear and myths.
Patients feel less lost.
They become active participants.
Physicians should introduce prosthetics early.
Even during acute care when appropriate.
This builds continuity.
Fitting should be delayed if wounds are unstable.
Severe pain or infection requires resolution first.
Psychological distress may also need support.
Delay should be explained clearly.
Patients should know it is temporary.
A plan should always be shared.
Delay without explanation harms trust.
Delay with purpose builds confidence.
Communication makes the difference.
Temporary devices allow early learning.
They accommodate limb changes over time.
They reduce pressure to be perfect.
Indications include changing limb shape or uncertain tolerance.
These devices guide final prescription decisions.
They are clinically valuable.
Physicians should support their use.
They are not inferior solutions.
They are part of good care.
One of the most important clinical questions in upper-limb prosthetic prescription is how the patient used their hands before limb loss. Hand dominance affects task habits, work skills, and daily routines in deep ways. Loss of the dominant hand often creates stronger indication for prosthetic prescription because the impact on independence is greater and more immediate.
However, dominance alone should not drive the decision. Many patients adapt by retraining the opposite hand, especially for fine tasks. Physicians should explore which activities now feel most limited and which adaptations the patient has already made. This conversation helps determine whether a prosthesis will meaningfully add function or simply duplicate what the patient has already learned to do without it.
Understanding hand use patterns allows physicians to align the prosthesis with real-life needs rather than assumed deficits.
Upper-limb prosthetic function depends heavily on the joints above the level of loss. Shoulder strength, stability, and range of motion are especially important, even in below-elbow amputations. Painful shoulders, rotator cuff disease, or severe stiffness can limit the ability to position and control a prosthesis.
Physicians should examine proximal joints carefully and not assume that distal limb loss is the only concern. In some cases, addressing shoulder pain or stiffness first can transform a poor prosthetic candidate into a good one. In other cases, severe joint disease may limit the benefit of complex devices and shift the indication toward simpler or cosmetic solutions.
Good joint health expands prosthetic options and improves long-term tolerance.
Residual limb pain, neuroma pain, or hypersensitivity can interfere with prosthetic use. These issues do not always contraindicate fitting, but they strongly influence timing and device choice. Persistent pain often leads to limited wear time and eventual abandonment if not addressed early.
Physicians should assess pain patterns carefully and distinguish between expected post-surgical discomfort and ongoing pathological pain. Early referral for pain management, desensitization, or surgical review may be needed before fitting proceeds. Ignoring pain rarely leads to adaptation and usually results in failure.
Comfort is not a luxury in upper-limb prosthetics. It is a prerequisite for use.
Upper-limb prosthetic use requires visual feedback and coordination, especially during early training. Patients with severe visual impairment, balance disorders, or neurological coordination issues may face higher risk during use. This does not automatically rule out prosthetic prescription, but it shapes expectations and safety planning.
Physicians should consider whether the patient can safely use a prosthesis during daily tasks such as cooking or tool use. When risks are identified, additional training, environmental modification, or caregiver involvement may be required. These factors should be discussed openly before prescription.
Safety awareness is as important as mechanical function.
One of the clearest indications for upper-limb prosthetic prescription is difficulty with basic self-care. Tasks such as eating, dressing, bathing, and personal hygiene often require two hands for efficiency and safety. When patients struggle with these tasks despite therapy and adaptation, prosthetic support becomes clinically justified.
Physicians should ask patients to describe specific moments of difficulty rather than general frustration. Details about spilling food, slow dressing, or unsafe bathroom transfers reveal where a prosthesis may help most. These concrete examples guide more effective prescriptions than abstract goals.
Restoring self-care independence often has strong psychological benefits alongside physical ones.
Work-related demands are a major driver of upper-limb prosthetic success. Patients who need to return to jobs involving tools, machinery, computers, or manual handling often have strong motivation to adapt to a prosthesis. In these cases, prescription is not only about function but also economic stability and identity.
Physicians should explore job requirements in detail, including hand positions, grip strength, repetition, and safety risks. This information helps prosthetic teams design task-specific solutions and prevents unrealistic expectations. Early alignment with vocational goals increases the chance of long-term use.
When work is central to the patient’s life, prosthetic prescription often becomes a priority.
Upper-limb loss can deeply affect social interaction. Hand gestures, greetings, and shared activities all play a role in communication and self-image. For some patients, social discomfort becomes a strong indication for prosthetic prescription, even if functional needs are modest.
Physicians should not dismiss these concerns as cosmetic or secondary. Social participation influences mental health, relationships, and quality of life. A prosthesis that restores confidence in public settings may provide meaningful benefit even if functional gains are limited.
Clinical care should respect social and emotional dimensions of recovery.
Hobbies such as cooking, music, sports, or crafts often shape a person’s sense of self. Loss of an upper limb can disrupt these activities in ways that deeply affect well-being. When a prosthesis can support return to valued hobbies, indication becomes strong.
Physicians should ask about activities that bring joy or purpose. These details often reveal motivation levels and willingness to train. When patients see a clear path back to meaningful activities, they engage more fully in rehabilitation.
Personal identity is a valid clinical consideration.
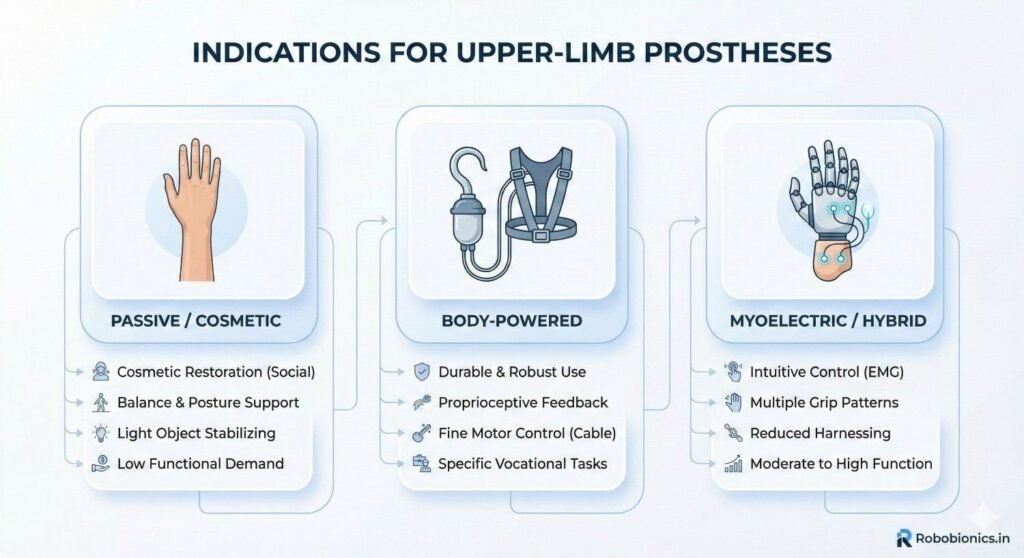
Mechanical or body-powered prostheses are often indicated when reliability, durability, and simplicity are priorities. Patients who work in demanding environments or prefer low maintenance may benefit most from these devices. They also suit individuals who want predictable function without reliance on batteries or electronics.
Physicians should consider these devices when patients have good shoulder movement and can tolerate harness systems. While function may be limited compared to advanced devices, consistent use often leads to better real-world outcomes.
Simplicity can be a strength, not a compromise.
Myoelectric prostheses are indicated when patients have good muscle signal control, cognitive capacity, and motivation for training. They can offer improved grip patterns and appearance, which may support both functional and social goals.
However, these devices require regular charging, maintenance, and structured training. Physicians should ensure that patients understand these demands clearly. Without realistic expectations, advanced devices are at higher risk of abandonment.
Appropriate indication balances potential benefit with capacity to manage complexity.
Passive prostheses serve important roles in balance, body image, and task stabilization. They are often indicated when active control is limited or when the primary goal is appearance and symmetry. These devices can support bimanual tasks by holding or bracing objects.
Physicians should recognize their clinical value and avoid framing them as lesser options. For many patients, passive solutions provide comfort and confidence that outweigh the benefits of more complex devices.
Matching the device to the goal is the essence of good prescription.
Many patients benefit from a staged approach, beginning with a simple device and progressing to more advanced options over time. Indications for staged care include uncertain tolerance, evolving goals, or changing medical status.
Physicians should present this pathway as intentional and flexible rather than indecisive. Staged approaches reduce pressure and allow learning without overwhelming the patient.
Adaptability supports long-term success.
Upper-limb loss often triggers grief, anger, or withdrawal. These responses are normal but can affect readiness for prosthetic training. Physicians should assess whether emotional distress is likely to interfere with learning or safety.
In many cases, prosthetic fitting itself supports emotional recovery by restoring agency. In others, counseling or peer support may be needed first. The decision should be individualized rather than rule-based.
Emotional readiness is dynamic and deserves attention.
Patients may believe a prosthesis will fully restore normal hand function or fear that it will be useless. Both beliefs can undermine success if left unaddressed. Physicians play a key role in shaping balanced expectations through honest conversation.
Clear explanations of what a prosthesis can and cannot do help patients engage realistically. When expectations align with reality, satisfaction improves even if function is limited.
Expectation management is a core clinical skill in prosthetic care.
Family attitudes can strongly influence acceptance. Supportive families encourage practice and persistence, while fearful or dismissive responses may hinder use. Physicians should assess family dynamics and include caregivers in discussions when appropriate.
Education reduces fear and builds shared understanding. When families understand the purpose and limits of a prosthesis, they become allies in care rather than sources of pressure.
Support systems often determine outcomes more than device type.
Upper-limb prosthetic prescription should never be automatic. In some situations, fitting a device can increase frustration, pain, or risk rather than improve function. Physicians must recognize when the expected benefit is low or when the patient’s current condition makes safe use unlikely.
Severe uncontrolled pain at the residual limb, active infection, or unstable wounds are clear reasons to delay fitting. Introducing a prosthesis in these situations often worsens symptoms and damages trust. In such cases, focusing on healing and comfort first leads to better long-term outcomes.
Knowing when to wait is as important as knowing when to act.
Upper-limb prostheses require learning, awareness, and safe decision-making during use. Patients with severe cognitive impairment, active psychosis, or persistent unsafe behavior may not be able to use a device safely, even with training. In these cases, prescription may place the patient at risk of injury.
This does not mean care stops. It means goals shift toward safety, caregiver support, and alternative strategies. Physicians should document reasoning clearly and revisit decisions if circumstances change.
Clinical caution protects dignity when framed with respect and honesty.
Some patients continue to believe that a prosthesis will function like a natural hand despite repeated explanations. Others reject all potential benefit and refuse training. When expectations remain fixed and extreme, prosthetic fitting often fails.
Physicians should invest time in education and peer exposure where possible. However, if insight does not improve, delaying prescription may prevent emotional harm and device abandonment. This is a relative contraindication that requires judgment rather than rigid rules.
Protecting patients from disappointment is part of good care.
A strong prescription explains what the prosthesis is meant to achieve in daily life. Rather than naming device types or brands, physicians should describe functional goals such as assisting with eating, stabilizing objects, or supporting return to work.
This approach gives prosthetists and therapists the flexibility to design the most appropriate solution. It also keeps the focus on outcomes rather than equipment.
Intent-driven prescriptions lead to better collaboration and results.
Physicians should include limb level, side, diagnosis, healing status, pain issues, and any precautions. Information about shoulder range, endurance, and cognitive considerations is also valuable.
Clear details reduce guesswork and prevent unsafe assumptions. They also speed up the fitting process and reduce unnecessary back-and-forth.
Clarity at this stage saves time later.
Upper-limb prosthetic prescription should always include a plan for review. Early follow-up allows adjustment, reassurance, and problem-solving before small issues grow larger.
Physicians should signal openness to revisiting decisions and modifying goals. This flexibility reassures patients and supports long-term engagement.
Prescription is the beginning of a process, not the end.
The first weeks after fitting are critical. Patients are learning new movement patterns and often feel awkward or slow. Physicians should normalize this phase and encourage persistence.
Early check-ins help identify pain, skin issues, or emotional distress. Addressing these early prevents abandonment and builds confidence.
Support during this phase often determines success.
Progress should be measured against the goals set at prescription. Improvement may be gradual, but it should be meaningful to the patient’s daily life. Physicians should ask whether the prosthesis is actually being used and for what tasks.
If use is limited, the reason should be explored without judgment. The solution may involve device adjustment, more training, or revised goals.
Listening closely improves care quality.
Over time, patients’ needs and abilities change. Weight changes, new work demands, or improved strength may indicate the need for device modification or upgrade. Conversely, declining health may shift goals toward comfort.
Physicians should view revision as a normal part of prosthetic care. Reassessment supports long-term relevance and satisfaction.
Flexibility keeps care patient-centered.
Upper-limb prosthetic indications in children depend on development, play needs, and family support. Early exposure can normalize prosthetic use, but devices must be simple and safe.
Physicians should focus on function and confidence rather than perfection. Frequent review is needed as children grow and goals change.
Family education is essential in pediatric care.
In older patients, upper-limb prosthetic goals often center on basic independence and confidence. Simpler devices and slower training are usually appropriate.
Physicians should avoid age-based assumptions and focus on functional ability and motivation. Many older adults benefit greatly when expectations are realistic.
Respecting pace improves acceptance.
Bilateral loss presents complex challenges and strong indications for assistive solutions. Prosthetic prescription should be staged and carefully planned.
Physicians should coordinate closely with rehab teams to balance safety, training load, and functional goals. Even partial prosthetic use can make a meaningful difference.
These cases require patience and teamwork.
Physician involvement should not end with referral or prescription. Continued engagement reinforces the importance of prosthetic care and reassures patients that they are supported.
Follow-up visits provide opportunities to reinforce goals and address concerns. This continuity improves adherence and satisfaction.
Presence matters.
Upper-limb prosthetic success depends on close collaboration between physicians, prosthetists, therapists, and mental health professionals. Physicians play a key role in aligning these voices.
Clear communication prevents mixed messages and unsafe decisions. Team-based care is the standard for complex rehabilitation.
Collaboration multiplies impact.
Physicians often influence whether patients receive timely prosthetic care. Advocacy for access, affordability, and appropriate technology is part of ethical practice.
When clinicians support equitable solutions, more patients benefit and outcomes improve across populations.
Access is a clinical issue, not just a policy one.
At RoboBionics, we work closely with physicians to understand when and why upper-limb prostheses should be prescribed. Our focus is on creating devices that align with real clinical indications, patient readiness, and daily life needs.
By keeping designs practical, affordable, and adaptable, we support physicians in making responsible prescribing decisions without pressure to overpromise.
Clinical judgment guides innovation, not the other way around.
We recognize that many patients benefit from staged prosthetic pathways. Our solutions support gradual progression, allowing patients to build confidence and skill over time.
This approach respects contraindications, readiness, and changing goals. It also improves long-term use and satisfaction.
Sustainable care is thoughtful care.
Our role extends beyond devices. We support training, follow-up, and collaboration so that physicians are not left to manage complex decisions alone.
When clinicians and technology partners work together, patients receive safer and more effective care.
Partnership strengthens outcomes.
Traumatic upper-limb loss often affects younger and working-age patients.
These patients usually have strong motivation to regain function and return to work.
The indication for prosthetic prescription is often clear, but timing must be thoughtful.
Soft tissue condition after trauma can be unpredictable.
Swelling, pain, and nerve sensitivity may persist longer than expected.
Physicians should balance early motivation with biological readiness.
Early referral is still important, even if fitting is delayed.
Education, limb shaping, and expectation setting can begin early.
This keeps momentum without increasing risk.
Upper-limb loss from infection or vascular causes often involves fragile tissue.
Healing may be slower and skin tolerance lower.
Indications for prosthetic fitting depend heavily on stability.
Physicians should wait for clear signs of durable healing.
Repeated breakdown after early fitting is common in these cases.
Patience improves long-term success.
Functional goals may also differ in this group.
Support for basic daily tasks may matter more than fine dexterity.
Device choice should reflect these priorities.
Cancer-related amputations often carry emotional and psychological weight.
Patients may be coping with fear, fatigue, or ongoing treatment.
Indications for prosthetic care must consider overall disease status.
When prognosis is stable and recovery is expected, prosthetic fitting can restore normalcy.
It can help patients reconnect with daily routines and identity.
In these cases, the benefit is often both functional and emotional.
If treatment is ongoing or energy is limited, goals may shift.
Cosmetic or passive prostheses may be more appropriate initially.
Physicians should revisit decisions as health status changes.
Congenital limb differences require a different indication framework.
These patients often adapt remarkably well without prostheses.
Prescription is not automatic and should never be forced.
Indications arise when function, symmetry, or social comfort becomes a concern.
This often happens during school age or adolescence.
Patient choice is especially important here.
Physicians should avoid comparing these patients to acquired amputees.
Their needs and adaptation patterns are different.
Respecting autonomy leads to better acceptance.
Upper-limb prosthetic abandonment is common when indications are weak.
This usually reflects mismatch between device and real-life need.
It is rarely due to patient failure.
Physicians should see abandonment as feedback, not non-compliance.
It signals that goals, timing, or expectations were off.
Reassessment can often restore value.
Early identification of low use is important.
Delayed response reduces chances of re-engagement.
Regular follow-up protects outcomes.
Long-term indication exists when the prosthesis is used regularly and meaningfully.
This may include daily self-care, work tasks, or social situations.
Use does not have to be constant to be valuable.
Physicians should ask how and when the prosthesis is used.
Even limited but purposeful use can justify continued care.
Value is defined by the patient’s life, not clinic metrics.
Continued prescription also depends on comfort and safety.
Persistent pain or injury may require revision.
Indication should always be reassessed.
Upper-limb prostheses wear out or become outdated.
Indications for replacement include poor fit, reduced function, or new goals.
Changes in work or lifestyle often drive this need.
Physicians should support timely replacement when benefit is clear.
Delaying too long can reduce function and confidence.
Upgrades should be goal-driven, not trend-driven.
Clear documentation helps justify these decisions.
Clinical reasoning matters for access and approval.
Consistency strengthens patient trust.
Many patients abandon upper-limb prostheses because success was never defined.
Physicians should explain what early success looks like in simple terms.
Slow progress and awkward movement are normal at first.
Setting short-term milestones helps patients stay engaged.
These may include wearing the device daily or completing one task independently.
Progress builds confidence over time.
Clear framing prevents unnecessary disappointment.
Patients who know what to expect persist longer.
Education supports resilience.
Upper-limb prosthetic use requires practice.
Muscle memory, coordination, and problem-solving take time.
This effort should be explained clearly before prescription.
Physicians should avoid minimizing the work involved.
Honest conversations build trust.
Patients are more willing when they feel respected.
Effort is not a sign of failure.
It is part of adaptation.
This message should be repeated often.
Patients should know that using a prosthesis is not a one-way decision.
They can pause, modify, or change devices if needed.
This flexibility reduces fear and pressure.
Physicians should normalize reassessment.
Changing plans reflects learning, not indecision.
Adaptability supports long-term engagement.
This mindset keeps care patient-centered.
It also reduces abandonment due to frustration.
Choice empowers patients.
Delayed referral is a common reason for poor outcomes.
Patients lose motivation or adapt in ways that reduce prosthetic benefit.
Early referral keeps options open.
Physicians should know local prosthetic pathways.
Clear referral processes reduce delays and confusion.
Systems matter as much as individual decisions.
Even when fitting is delayed, referral should not be.
Planning can begin early.
This improves continuity of care.
Cost influences access and adherence.
Prescribing a device that a patient cannot maintain creates harm.
Affordability is a clinical consideration.
Physicians should discuss costs openly and honestly.
Multiple options should be explored.
The best device is the one the patient can use long-term.
Balancing function and cost requires judgment.
There is no single right answer.
Transparency builds trust.
Access to upper-limb prosthetics varies widely.
Geography, income, and awareness all play a role.
Physicians are often gatekeepers to care.
Advocating for appropriate referral and support improves equity.
Simple, effective devices can change lives when used well.
Equity starts with thoughtful indication.
Clinical care should not be limited by assumptions.
Each patient deserves fair evaluation.
This is part of ethical practice.
What physicians say early after limb loss matters deeply.
Hopeful but honest language shapes how patients see prosthetics.
Dismissive or rushed conversations cause long-term harm.
Physicians should speak with clarity and empathy.
Avoid absolutes and false promises.
Balanced guidance builds trust.
Patients often remember these early discussions for years.
They influence willingness to try.
Language is a clinical tool.
Upper-limb prosthetic success is not achieved in one visit.
Ongoing physician involvement reinforces importance and support.
Even brief check-ins can make a difference.
Patients feel less alone when their doctor stays engaged.
This improves adherence and satisfaction.
Presence strengthens outcomes.
Care continuity matters more than device features.
Relationships support recovery.
This cannot be outsourced.
Physicians must sometimes advocate against pressure.
Pressure to rush fitting or prescribe complex devices is real.
Patient-centered judgment must guide decisions.
Saying no or wait can be the right care.
So can saying yes with support.
Clinical courage protects patients.
Thoughtful indication is a mark of good medicine.
It balances risk and hope.
This balance defines quality care.
Upper-limb prosthetic indication should not feel like a rare or complex decision reserved for specialists. It can be integrated into routine clinical thinking when physicians consistently ask the right questions about function, goals, and readiness. Over time, this approach becomes intuitive rather than time-consuming.
When indication assessment is part of standard review after limb loss, referrals become timely and purposeful. Patients feel guided rather than uncertain. This consistency improves outcomes across settings, from tertiary centers to smaller hospitals.
Good habits simplify complex care.
While guidelines are helpful, upper-limb prosthetic indication works best through conversation rather than rigid checklists. Asking patients how their daily life has changed, what frustrates them most, and what they hope to regain provides richer insight than scoring tools alone.
Physicians should listen more than they speak in these discussions. Patients often reveal readiness, motivation, or hesitation through stories rather than direct answers. These cues guide safer and more effective decisions.
Clinical listening is a powerful diagnostic tool.
Physicians do not need all the answers before referring to prosthetic services. Early referral allows multidisciplinary teams to assess options together. Waiting for perfect clarity often delays care unnecessarily.
If there is a reasonable chance that a prosthesis could improve function or quality of life, referral is appropriate. Final decisions can evolve through collaboration.
Shared assessment reduces individual burden.
This belief persists because poorly indicated prostheses often go unused. When devices are prescribed without clear goals or readiness, abandonment follows, reinforcing the myth. In reality, well-indicated upper-limb prostheses provide meaningful benefit to many patients.
Physicians who see successful cases understand that usefulness depends on timing, intent, and support. Challenging this myth starts with better indication, not lower expectations.
Usefulness is created, not assumed.
Many patients do not know what is possible. They may assume prosthetic care is not available or not meant for them. Waiting for patients to ask often means missing the window of readiness.
Physicians should introduce the option proactively and neutrally. This empowers patients to consider choices they may not have imagined.
Silence limits access.
Technology alone does not determine success. Advanced upper-limb prostheses require training, maintenance, and commitment. When these demands exceed patient capacity, simpler devices perform better in real life.
Physicians should focus on matching device complexity to patient readiness. The right solution is the one that will be used, not admired.
Appropriateness matters more than innovation.
Physicians build confidence by seeing outcomes over time. Following patients after prescription, observing what works and what does not, sharpens judgment more than any guideline.
Each case adds to clinical intuition. Reflecting on both successes and failures strengthens future decisions.
Experience is a powerful teacher.
Prosthetists and therapists see daily patterns of use and abandonment. Their feedback helps physicians refine indication decisions. Open communication creates a learning loop that benefits future patients.
Physicians should welcome this feedback rather than seeing it as critique. Shared insight improves care quality.
Collaboration builds confidence.
Upper-limb prosthetic care is evolving. New designs, training methods, and support systems continue to emerge. Indication principles remain stable, but application adapts with experience.
Physicians who remain curious and flexible provide better care over time. Rigidity limits growth.
Adaptability supports excellence.
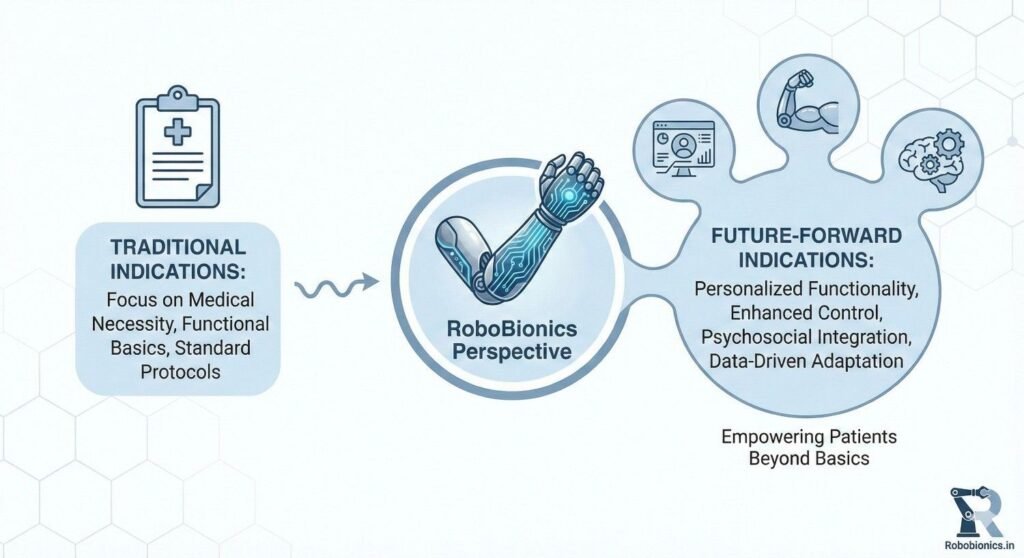
At RoboBionics, we design upper-limb prosthetic solutions around real clinical indications rather than idealized use cases. Our experience across India has shown that devices succeed when they respect patient readiness, lifestyle, and support systems.
We work closely with physicians to understand when prescription makes sense and when staged or simplified approaches lead to better outcomes. This alignment reduces abandonment and improves long-term use.
Clinical reality guides our innovation.
We recognize that prescribing an upper-limb prosthesis is only one step in a longer journey. That is why we support training, patient education, and follow-up alongside device delivery.
Our goal is to make it easier for physicians to prescribe responsibly, without pressure to overpromise or rush fitting. Support systems matter as much as technology.
Partnership strengthens patient care.
Affordability plays a major role in whether upper-limb prosthetic care is sustained. By focusing on locally made, cost-effective solutions, we help physicians recommend options that patients can realistically maintain.
This reduces ethical tension around prescribing devices that patients may not be able to afford or service. Access and dignity should go hand in hand.
Sustainable care is equitable care.
Upper-limb prosthetic prescription is one of the most nuanced decisions a physician can make in rehabilitation care. It requires balancing medical readiness, functional need, psychological factors, and long-term support. When indications are clear and patient-centered, prosthetic care becomes a powerful tool for restoring independence and confidence.
The most successful outcomes come from thoughtful timing, honest communication, and ongoing involvement. Upper-limb prostheses are not for everyone, but for the right patient at the right time, they can change the course of recovery.
By grounding decisions in real-life function and collaboration, physicians can ensure that upper-limb prosthetic prescription is safe, ethical, and meaningful. At RoboBionics, we are committed to supporting this approach, working alongside clinicians to help more people regain function, dignity, and hope through responsible prosthetic care.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body