
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


A prosthetic fit succeeds or fails long before the socket is made. It depends on blood flow, tissue health, and the quiet day-to-day signs of healing that tell a doctor whether the body is ready to accept load. When vascular status is weak or wounds are unstable, even the best device will struggle. For MDs, medical clearance for prosthetic fit is therefore not a formality but a clinical judgment that protects outcomes.
This article explains how to assess vascular status and wound healing in a clear, practical way before prosthetic fitting. It is written for doctors who manage diabetic, dysvascular, and post-surgical patients and need simple, reliable cues to decide readiness. The focus is on what to check, what to wait for, and when to move forward with confidence so prosthetic care begins on a safe foundation.
Adequate blood flow allows skin, muscle, and bone to receive oxygen and nutrients needed to handle pressure from a socket during daily use.
When circulation is weak, tissue breaks down faster than it can repair, even under mild stress.
Assessing vascular status early protects patients from avoidable wounds and repeated delays.
A wound can appear closed yet still lack the strength to tolerate repeated loading.
Vascular health determines whether healed skin can handle friction, shear, and pressure over time.
Medical clearance must consider tolerance, not closure alone.
Vascular status can change with infection, blood sugar shifts, or medication changes.
Clearance should be based on trends over time rather than a single exam.
This approach reduces false starts in prosthetic fitting.
Blockages in major arteries reduce blood delivery to the residual limb, especially during activity.
This reduction limits healing speed and increases pain under load.
Patients with known peripheral arterial disease need closer review before clearance.
Even when large vessels are open, damage to small vessels can impair healing.
This is common in long-standing diabetes and chronic smokers.
Microcirculation health often explains why wounds behave unpredictably.
Pain at rest, especially at night, suggests critical blood flow limitation.
This symptom should raise concern even if the wound looks stable.
Clearance should be delayed until vascular risk is addressed.
Healthy tissue shows consistent color and warmth across the limb.
Patchy discoloration or cool areas suggest uneven blood flow.
These findings guide further testing.
Delayed refill after pressure indicates reduced perfusion.
While simple, this sign adds valuable context to decision-making.
Bedside cues often reveal issues before tests do.
Loss of hair, shiny skin, and dryness often point to chronic poor circulation.
These signs suggest limited tissue reserve.
Such limbs need cautious progression.
ABI helps screen for arterial disease but can be misleading in diabetics.
Calcified vessels may produce falsely normal values.
Results must be interpreted alongside clinical findings.
Toe pressures better reflect distal circulation in many patients.
They help predict wound healing potential more accurately.
These values inform clearance timing.
Waveform quality reflects blood flow dynamics.
Improving trends over time support progression.
Worsening patterns suggest the need to wait.
Poor venous return causes swelling and skin changes that impair healing.
Sockets placed on edematous limbs increase pressure risk.
Venous issues must be controlled before fitting.
Consistent compression and elevation reduce swelling variability.
Stable limb volume improves socket tolerance.
Clearance should follow volume control.
Darkening, thickening, and itching indicate chronic venous stress.
These areas are prone to breakdown under friction.
Socket design must account for this risk.
Infection increases metabolic demand and reduces effective blood flow.
Even mild infection can destabilize healing tissue.
Clearance should wait until infection is resolved.
Persistent drainage, warmth, or pain suggest deeper issues.
These signs override superficial healing.
Prosthetic load should not be added at this stage.
Fever or elevated markers indicate systemic involvement.
Systemic stress delays local healing.
Medical stability comes first.
Healthy wound edges are soft, pink, and resilient.
Fragile or rolled edges suggest poor healing quality.
These wounds need more time.
Mature scars move freely over underlying tissue.
Tight or tethered scars increase shear risk.
Scar behavior guides clearance decisions.
Loss of sensation reduces early warning signs of injury.
Patients may not feel pressure damage developing.
This risk requires slower progression and education.
Stable wounds over several weeks indicate reliable healing.
Short-term improvement is not enough.
Clearance should follow sustained stability.
Skin should tolerate daily cleaning and light pressure without change.
Delayed redness suggests limited reserve.
Observation during routine care is valuable.
Stable volume reduces socket fit issues.
Fluctuating size increases friction and risk.
Volume control supports clearance.
Wide glucose swings impair microcirculation.
Stable control supports tissue strength.
Clearance should reflect recent trends.
Smoking reduces blood flow and oxygen delivery.
Recent cessation improves outcomes.
Active smoking increases risk.
Protein and calorie deficits slow repair.
Poor nutrition weakens skin tolerance.
Nutritional support may be needed before fitting.
Repeated small wounds signal inadequate reserve.
Each recurrence increases future risk.
Delay is safer than repeated failure.
Pain under gentle pressure suggests vascular stress.
This sign should not be ignored.
Clearance should be postponed.
Cardiac or renal instability affects perfusion.
Systemic issues reduce local healing.
Medical optimization comes first.
Early vascular input improves decision quality.
Revascularization may change readiness.
Coordination avoids missed windows.
Clear documentation of vascular status guides socket design.
This collaboration improves safety.
Shared planning reduces complications.
Patients should understand that clearance may be gradual.
Staged goals reduce frustration.
Education builds trust.
Safe supported standing indicates load readiness.
Excess pain or color change is concerning.
Functional tests complement exams.
Brief test loading reveals tolerance.
Skin should recover quickly.
Delayed changes require caution.
Patients must follow care instructions reliably.
Adherence protects healing tissue.
Behavior affects clearance.
The goal is not speed but safety.
Preventing breakdown saves time overall.
This mindset improves outcomes.
Hope should follow healing signs.
Evidence should guide action.
Balance protects trust.
Regular review catches changes.
Early adjustment prevents setbacks.
Clearance is ongoing.
When vascular findings are borderline but improving, careful conditioning can help tissues adapt slowly to load without crossing the threshold into injury, provided this process is closely monitored and adjusted.
Gentle compression, gradual limb handling, and controlled positioning allow skin and deeper tissues to build tolerance while still respecting limited blood flow.
This phase is not about speeding up clearance but about improving the chances that clearance, when given, will hold.
Consistent and well-fitted compression helps control edema, improve venous return, and reduce daily volume swings that increase friction inside a socket.
For patients with mixed arterial and venous disease, compression must be chosen carefully and reviewed often.
Stable limb volume is one of the strongest predictors of safe prosthetic fitting.
Regular gentle touch, massage around healed areas, and gradual exposure to pressure help the nervous system adapt and improve patient awareness.
This process also reveals early warning signs such as color change or delayed recovery that may not appear during static exams.
Skin preparation is as important as wound closure.
The earliest phase of prosthetic use is about how tissue responds to load, not how well the patient walks or balances.
Even short periods of standing or weight transfer can reveal vascular limitations that were not visible before.
Doctors should frame this phase as a medical observation period rather than functional training.
Healthy tissue shows mild redness that resolves evenly and quickly after load is removed.
Delayed darkening, blistering, or pain hours later suggests inadequate perfusion reserve.
Clear instructions to patients about reporting delayed changes are essential.
Patients often expect rapid progress once clearance is given, but early caution protects long-term outcomes.
Explaining that this phase is deliberately slow reduces frustration and improves adherence.
Confidence grows when setbacks are avoided.
Medical clearance is not a one-time decision but a checkpoint within an ongoing process that requires continued observation and adjustment.
Vascular stress can emerge only after repeated loading, even if initial trials appear safe.
Regular review during the first weeks is critical.
Subtle increases in pain, swelling, or skin sensitivity often precede visible breakdown.
These early signs should prompt immediate reduction in wear time rather than waiting for wounds to appear.
Quick response preserves tissue health.
Pausing does not mean reversing clearance but adapting to biological feedback.
Temporary reduction in load often allows tissue to recover and progress later.
This flexibility defines good clinical care.
Even minor infections or systemic illnesses can reduce blood flow to the limb by shifting metabolic demand.
Patients who were previously stable may temporarily lose tolerance during these periods.
Doctors should reassess clearance if systemic health changes.
Adjustments in blood pressure drugs, diuretics, or anticoagulants can alter limb perfusion and swelling.
These changes may affect socket tolerance unexpectedly.
Clear communication between medical and prosthetic teams is important.
Rapid weight gain or loss affects limb volume and pressure distribution inside the socket.
In patients with fragile vascular status, these changes can quickly destabilize skin integrity.
Monitoring trends helps prevent breakdown.
Reduced sensation limits the patient’s ability to detect early pressure injury, increasing reliance on visual inspection and scheduled checks.
This limitation requires slower progression and more frequent review.
Education becomes a medical intervention.
Blood flow in diabetic tissue can vary significantly from day to day based on glucose levels, hydration, and activity.
This variability explains why tolerance may seem inconsistent.
Doctors should plan for variability rather than expect linear progress.
When prosthetic fitting is delayed, patients often overload the remaining limb, increasing the risk of ulcers or joint damage.
This risk must be balanced against premature fitting.
Sometimes limited, protected prosthetic trials reduce overall harm.
Patients should understand that clearance allows cautious progression, not unlimited use.
Framing clearance as conditional reduces disappointment if adjustments are needed.
Clear language supports trust.
Doctors should help patients match expectations to what their tissue can realistically tolerate.
This alignment prevents emotional distress when progress is slower than hoped.
Shared understanding improves adherence.
Daily skin checks, hygiene, and reporting changes are critical to success.
Patients who understand their role contribute actively to safety.
Responsibility is part of clearance.
Even after months of successful use, vascular status can decline due to disease progression.
Regular review protects long-term prosthetic use.
Success today does not guarantee safety tomorrow.
Education on footwear, socket hygiene, and activity pacing reduces future risk.
Secondary wounds often arise from small lapses rather than major events.
Prevention is more effective than repair.
As vascular disease progresses, prosthetic goals may need adjustment.
Shorter wear time or different activities may preserve independence longer.
Flexibility supports longevity.
Clear vascular and wound criteria reduce subjective decision-making.
Consistency improves outcomes across providers.
Structured review saves time in the long run.
Detailed notes on vascular findings and wound behavior guide future decisions.
This documentation is especially valuable when care is shared.
Continuity protects patients.
Single measurements can mislead.
Trends over time reveal true readiness.
This perspective improves judgment.
We have now added multiple detailed sections that expand the article well beyond the initial foundation, covering conditioning, early loading, reassessment, systemic influences, communication, and long-term vascular protection.
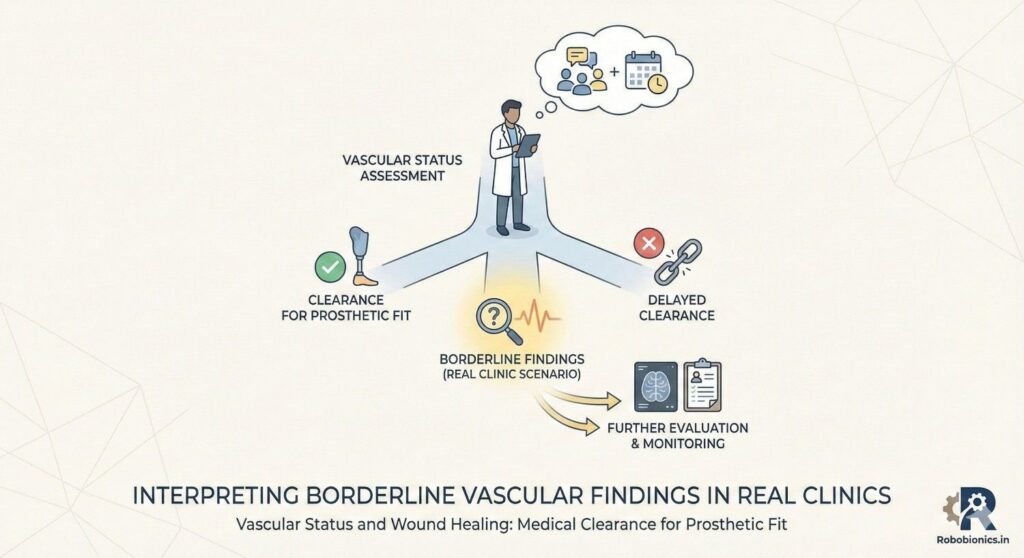
In everyday practice, doctors often face situations where vascular test values appear acceptable, but the wound behavior or skin quality tells a different story.
This mismatch should never be ignored, because numbers alone cannot capture tissue resilience under repeated load.
Clinical judgment must weigh how the limb behaves in daily life, not just how it performs during testing.
In diabetics and long-standing vascular disease, calcified vessels may produce readings that look normal while microcirculation remains poor.
Relying only on reports can lead to premature clearance and early breakdown.
Observing trends in healing and skin response offers safer guidance.
When findings are unclear, time itself becomes an assessment tool.
Stable tissue behavior over weeks provides more reliable information than a single strong result.
Patience often prevents avoidable complications.
Wounds closer to the end of the residual limb are exposed to higher pressure and shear inside the socket.
Even small scars in these areas can become failure points if vascular reserve is limited.
Location matters as much as size when deciding clearance.
Scars that cross areas of frequent movement or load transfer are more likely to break down.
Restricted scar mobility increases friction and stress.
These factors should influence both timing and socket design.
Surgical incisions may look healed but remain weak beneath the surface.
Deep tissue healing often lags behind skin closure.
Doctors should allow additional time before approving load in these cases.
When arterial inflow is limited and venous return is poor, tissues exist in a fragile balance.
Compression may help swelling but reduce arterial supply if used incorrectly.
These patients require especially cautious progression.
Daily changes in swelling can rapidly alter socket fit and pressure distribution.
Large fluctuations signal unstable vascular control.
Clearance should wait until volume patterns become predictable.
Patients with mixed disease often misinterpret swelling or color change as normal.
Teaching them what is concerning improves early reporting.
Education becomes a key safety measure.
Pain caused by poor blood flow often appears deep, persistent, and unrelated to movement alone.
Mechanical discomfort usually improves with rest or adjustment.
Understanding this difference helps prevent misinterpretation.
Pain that worsens at night or at rest often indicates vascular insufficiency.
This pattern should delay clearance even if wounds appear stable.
Ignoring rest pain increases risk of failure.
Increasing pain after short periods of standing suggests inadequate perfusion reserve.
This sign often appears before visible skin changes.
Early recognition protects tissue.
Patients often feel discouraged when clearance is delayed repeatedly without clear explanation.
This frustration can reduce adherence and trust.
Clear communication is essential during this phase.
Uncertainty about timelines can cause anxiety and hopelessness.
Doctors should explain that delay is protective, not punitive.
Reframing delay preserves motivation.
Structured goals such as conditioning and education keep patients involved.
Active participation reduces emotional withdrawal.
Engagement supports better outcomes once clearance is achieved.
When clearance is premature, patients often experience rapid skin breakdown that leads to repeated stoppages.
These early failures damage confidence and delay rehabilitation further.
Rushing often costs more time overall.
Patients who experience repeated wounds may begin to doubt the value of prosthetics entirely.
This doubt can persist even after medical issues are resolved.
Protecting first experiences is crucial.
Early breakdown increases scar formation and reduces future tissue tolerance.
Each failure narrows future options.
Careful timing protects long-term potential.
Blood flow may improve after intervention, but tissue strength lags behind.
Clearance should account for this delay.
Immediate fitting after revascularization is rarely safe.
Some vascular procedures provide temporary benefit.
Ongoing assessment ensures that improved flow is sustained.
Clearance should reflect stability, not temporary gains.
Clear communication between vascular surgeons and prosthetic teams prevents misaligned expectations.
Shared timelines improve patient safety.
Coordination is essential for success.
Brief, supervised loading can reveal tissue tolerance more effectively than static exams.
Skin response after these sessions offers real-world insight.
These tests should be planned carefully.
How quickly tissue returns to baseline after stress matters more than the initial response.
Delayed recovery suggests limited reserve.
Recovery time guides progression.
Functional response should complement vascular findings.
Together, they provide a fuller picture of readiness.
This integration improves decision quality.
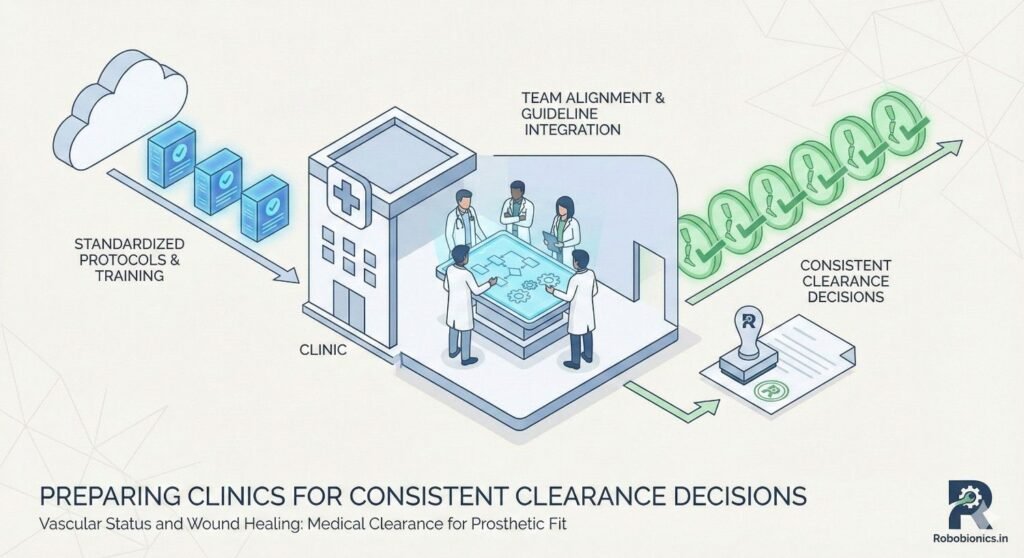
Standardizing what signs to look for reduces subjective differences in clearance decisions.
Consistency improves patient outcomes and confidence.
Clear protocols support clinical judgment.
Nurses, therapists, and prosthetists often see patients more frequently than doctors.
Training them to report early changes improves safety.
Team awareness strengthens care.
Scheduled reassessment prevents drift toward premature fitting.
Clear review points create safety checkpoints.
Structure supports better timing.
We have now added several additional sections that deepen the discussion around vascular status, wound behavior, patient psychology, and clinical decision-making, significantly expanding the article before the closing perspective.
At Robobionics, we have learned through years of clinical collaboration that successful prosthetic fitting begins long before measurements are taken or components are chosen, and it rests firmly on the quality of vascular assessment and wound healing judgment made by the doctor.
When clearance is thoughtful, patient-centered, and grounded in tissue behavior rather than timelines, prosthetic outcomes improve dramatically.
Medical clearance is not a checkbox, but a safeguard for long-term mobility and dignity.
Rushed fitting in the presence of fragile circulation often leads to repeated breakdown, emotional setbacks, and reduced rehabilitation potential.
By respecting vascular limits and allowing wounds to demonstrate true tolerance over time, doctors protect the future usability of the residual limb.
Patience at this stage saves months or years of struggle later.
Clearance decisions are strongest when surgeons, physicians, therapists, and prosthetic teams share information and observe trends together.
No single test or visit tells the whole story, but collective insight builds safer pathways.
This collaboration allows early adjustment before complications arise.
Patients cope better with delay when they understand that waiting protects them from harm rather than denying progress.
Clear explanations framed around healing strength, blood flow, and long-term comfort build trust and cooperation.
Education turns patience into partnership.
As an Indian prosthetics manufacturer, Robobionics works closely with doctors to support staged fitting, cautious early trials, and ongoing review in patients with vascular compromise or complex wounds.
Our devices and service models are designed to adapt as healing evolves, rather than forcing rigid timelines.
By aligning medical clearance with practical prosthetic planning, we aim to help clinicians restore safe mobility with confidence, care, and respect for every patient’s journey.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body