
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Returning to work after a serious injury or limb loss is not just about healing the body. It is about trust, safety, confidence, and function coming together at the right time. Doctors are often asked one simple question: “Is this person ready to work again?” The answer is rarely simple. This article explains how return-to-work decisions should be made, what functional signs truly matter, and how doctors can assess readiness in a way that protects dignity, productivity, and long-term health.
Returning to work is often treated like a yes or no decision. In reality, it is a layered process that needs careful thought.
A person may look healed on the outside but still struggle with strength, balance, or endurance.
Doctors must look beyond reports and scans to understand real work readiness.
When people return too early, injuries can worsen. Pain may increase and confidence can drop.
This often leads to repeated sick leave or job loss.
A slow, well-judged return protects both health and career.
Waiting too long also has risks. Skills may fade and confidence may reduce.
People may begin to doubt their ability to work at all.
The goal is not speed or delay, but correct timing.
Two people with the same job title may do very different work.
One may sit at a desk, while another may move, lift, or travel often.
Doctors must understand the actual tasks, not just the role name.
Some jobs require standing for long hours. Others need fine hand control or strength.
Understanding how often tasks are repeated is important.
Small movements done all day can cause more strain than heavy work done rarely.
Work also demands focus, decision-making, and stress handling.
Pain, fatigue, or fear of re-injury can affect these abilities.
A return-to-work plan must consider mental readiness too.
A bone may heal, or a wound may close, but function may still be limited.
Stiffness, weakness, or loss of control can remain.
Doctors must assess what the person can actually do, not just what has healed.
Clinic tests are done in controlled spaces. Work happens in real, often messy environments.
Uneven floors, noise, heat, and pressure all affect performance.
Functional testing should reflect real work conditions as much as possible.
How a person moves matters more than how much they can lift once.
Poor movement patterns can lead to new injuries.
Doctors should watch posture, balance, and effort closely.
Strength tests often focus on short bursts of effort.
Work usually requires steady effort over hours.
Endurance is often the missing piece in return-to-work decisions.
Fatigue can change how the body moves and reacts.
A person may start strong but lose control as they tire.
Doctors should assess performance over time, not just at the start.
Not every job needs high strength.
Doctors should match measured strength to actual job demands.
This avoids both overestimation and unnecessary restriction.
Limited joint movement can force the body into unsafe positions.
This increases the risk of strain or falls.
Work readiness depends on safe movement, not perfect movement.
Full range of motion is ideal, but functional range may be enough.
Doctors should ask if the available movement supports job tasks.
This practical approach helps realistic decision-making.
Many injuries occur when joints move beyond control.
Doctors should assess how well a person controls movement limits.
This is especially important for lifting and reaching tasks.
Pain does not always mean damage, but it affects performance.
Ignoring pain reports can harm trust between doctor and patient.
Pain should be understood, not dismissed.
Some pain may be manageable during work.
Other pain may reduce focus or strength.
Doctors should help patients identify safe pain levels.
Pain that increases steadily with activity is a warning sign.
Pain that settles with rest may be manageable.
These patterns guide safe return planning.
Balance affects how we sit, stand, and move.
Poor balance increases fall risk, even indoors.
Doctors should not ignore balance in return-to-work checks.
Some jobs need precise hand or foot control.
Coordination issues can reduce work quality and safety.
Simple coordination tests can reveal hidden challenges.
Slow reactions increase accident risk.
Fatigue, pain, or medication can affect alertness.
Doctors should consider these factors carefully.
Pain and stress can reduce focus.
Some medications may cause drowsiness.
Cognitive readiness is as important as physical readiness.
Work often involves quick choices.
Doctors should assess how stress affects the person.
Simple discussions can reveal readiness levels.
Complex jobs need memory and planning.
Injuries and trauma can affect these skills.
These areas should not be overlooked.
Braces, supports, or prosthetics can improve function.
They may reduce strain and improve safety.
Doctors should assess work readiness with these devices in place.
Using a device well takes practice.
Return-to-work should not start before comfort is achieved.
Training reduces errors and builds confidence.
Not all devices suit all jobs.
Doctors should confirm that devices match work demands.
Regular review improves long-term outcomes.
A supportive workplace can bridge functional gaps.
Poor environments increase risk and stress.
Doctors should ask about workplace conditions.
Simple changes can make a big difference.
Task rotation, seating changes, or tool modification help.
Doctors can guide these decisions.
Clear communication reduces misunderstanding.
Doctors play a key role in setting realistic expectations.
This protects both worker and employer.
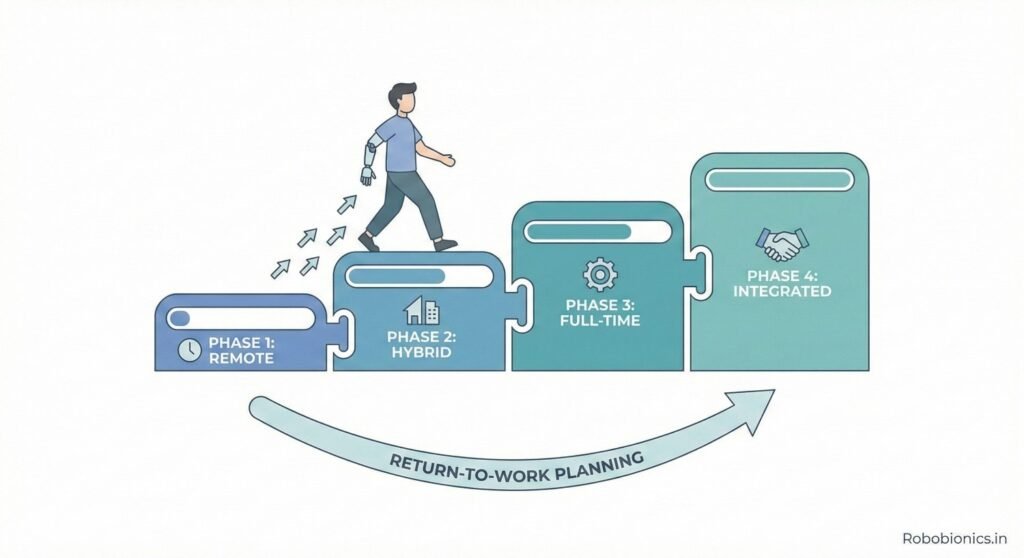
Starting full-time work suddenly can overwhelm the body.
Phased return allows adaptation.
This reduces injury and burnout risk.
Return-to-work is not a one-time decision.
Regular check-ins help adjust plans.
Flexibility improves success rates.
Setbacks can happen.
Doctors should encourage reporting issues early.
Timely adjustments prevent long-term problems.
Success is not just attendance.
Quality, safety, and comfort matter.
Doctors should assess these outcomes.
Confidence affects performance.
Fear can limit ability even when physically ready.
Doctors should ask about emotional state.
The goal is not short-term return.
Work should be sustainable without harming health.
This defines true success.
Muscle and joint injuries often heal on scans before function fully returns. Stiffness, weakness, and fear of movement can stay longer.
Doctors should assess how smoothly the person moves during work-like actions. Jerky or guarded movement often signals incomplete readiness.
Work tasks that involve repetition need special attention, as small limits can grow into big problems over time.
Nerve injuries heal slowly and sometimes unevenly. Strength may return without control, or sensation may remain altered.
Doctors should assess fine control, grip quality, and reaction to unexpected movement. These are critical for safe work.
Return-to-work decisions must remain flexible, as nerve recovery can change over months.
For people using prosthetics, work readiness depends on skill, comfort, and trust in the device.
Doctors should assess work tasks with the prosthetic in place, not without it.
True readiness comes when the person uses the device naturally, without constant mental effort.
Strong grip does not always mean useful grip. Control matters more than force in most jobs.
Doctors should observe how objects are held, released, and adjusted.
Dropping or crushing objects signals poor functional control.
Hands are often used continuously at work. Short tests may miss fatigue-related issues.
Doctors should assess performance over longer task periods.
Endurance failure often appears only after repeated use.
Reduced sensation increases injury risk. Heat, sharp edges, or vibration may go unnoticed.
Doctors should assess protective sensation and awareness.
Work may need adjustments if sensation is reduced.
Many jobs involve walking more than people realize.
Doctors should assess walking over time and on uneven surfaces.
Fatigue-related limping increases injury risk.
Standing for long hours stresses joints and spine.
Doctors should assess posture changes over time.
Pain or shifting weight often signals limited tolerance.
For lower limb prosthetic users, fit and comfort matter greatly.
Doctors should assess gait with real footwear and work conditions.
Confidence in movement predicts long-term success.
Fatigue is common after injury, even when strength returns.
It affects focus, reaction, and mood.
Doctors should ask about daily energy patterns.
Some jobs drain energy faster than others.
Doctors should match energy levels to job rhythm.
This prevents burnout and setbacks.
Work plans should include rest breaks when needed.
Ignoring recovery needs reduces long-term work ability.
Doctors should guide realistic pacing.
Fear can limit movement more than physical limits.
Doctors should listen carefully to these concerns.
Gradual exposure builds confidence safely.
Injury can affect how people see themselves at work.
Doctors should assess confidence in handling job demands.
Supportive planning rebuilds professional identity.
Work stress can worsen pain and fatigue.
Doctors should assess stress handling ability.
Mental readiness protects physical recovery.

Pain or fatigue can reduce patience and clarity.
Some injuries affect speech or expression.
Doctors should consider these factors for client-facing roles.
Supportive teams ease return-to-work.
Doctors can encourage open discussion with employers.
Good communication prevents misunderstandings.
Clear role expectations reduce pressure.
Doctors help by setting realistic limits.
This protects trust on all sides.
Doctors must protect patients from harm.
Approving return too early can cause damage.
Safety must come before pressure.
An unready worker may endanger others.
Doctors must consider wider impact.
This makes assessment even more important.
Written guidance helps employers act responsibly.
Vague notes create confusion.
Clarity protects everyone involved.
No single test defines readiness.
Doctors should combine observation, reports, and discussion.
A holistic view leads to better decisions.
Readiness changes with recovery and work exposure.
Regular reassessment improves outcomes.
Return-to-work is a process, not an event.
Patients often sense limits before tests show them.
Doctors should value this insight.
Trust improves honesty and outcomes.
Pain increase, fatigue, or reduced performance signal issues.
Doctors should encourage early reporting.
Timely action prevents setbacks.
Jobs may need further modification.
Doctors should remain involved beyond clearance.
Flexibility supports sustainability.
Some injuries change long-term capacity.
Doctors can help plan realistic career paths.
This protects dignity and income.
Doctors should work with therapists and prosthetists.
Shared insight improves assessment accuracy.
Teamwork benefits the patient most.
Rehabilitation should mirror real work.
This prepares the body and mind together.
Doctors can guide this focus.
The shift should be smooth, not sudden.
Clear handover reduces confusion.
This supports confidence.

Activity data can show real endurance levels.
Doctors can use this to guide decisions.
Objective data supports judgement.
Simulated tasks reveal hidden limits.
They bridge the gap between clinic and workplace.
Doctors should use them when possible.
Remote check-ins improve monitoring.
This is useful for long-term guidance.
Care continues beyond the clinic.
Success includes comfort, safety, and confidence.
Working without fear matters.
Doctors should define success broadly.
Short-term return is not enough.
Work should be maintainable for years.
This is the real goal.
Work is part of life, not all of it.
Doctors should align decisions with personal goals.
This keeps care human.
Medical reports often show healing, but they do not show how a person moves or copes during a full workday.
Doctors who rely only on reports may miss hidden risks.
Observation and discussion are just as important as test results.
Some patients underreport problems due to fear of losing their job.
Others may overstate ability out of pressure to return.
Doctors should create a safe space for honest conversation.
Many see clearance as the end of care.
In reality, it is the start of a new phase.
Ongoing support reduces failure rates.
Therapy sessions are planned and controlled.
Workdays are long and unpredictable.
Gradual exposure helps the body adjust safely.
One good day does not mean full readiness.
Doctors should look for consistent performance.
Patterns matter more than single results.
Needing more time is not failure.
Doctors should reinforce this message.
Confidence grows when pressure reduces.
Supportive workplaces improve outcomes.
Simple understanding reduces stress.
Doctors can encourage this culture.
Ignoring restrictions can cause re-injury.
Employers should follow recommended limits.
Clear communication helps compliance.
Return-to-work is a shared process.
Doctors, employers, and workers all play roles.
Shared goals improve success.
Many workers return early due to financial stress.
Doctors should understand this reality.
Sensitive planning is needed.
Many jobs lack formal safety measures.
Doctors should ask detailed questions.
Advice must match real conditions.
Doctors can help reframe recovery as strength.
This supports mental health.
Not all devices suit all tasks.
Doctors should assess function in real conditions.
This avoids misuse and frustration.
Using devices well takes time.
Return-to-work should follow skill mastery.
This improves safety.
Work demands may change.
Devices should adapt accordingly.
Regular review is essential.
Some injuries change capacity permanently.
Doctors should communicate this gently.
Honesty helps planning.
Role changes or new careers may be needed.
Doctors can guide realistic choices.
This protects dignity.
Career change can be painful.
Doctors should acknowledge this loss.
Support eases adjustment.
Reports should guide action, not confuse.
Specific limits help employers plan.
Clarity reduces conflict.
Words like “light duty” mean different things.
Doctors should define terms clearly.
Precision improves safety.
Conditions change with time.
Reports should reflect current ability.
Regular updates support trust.
Many doctors are not trained in work-focused evaluation.
Training improves confidence and accuracy.
This benefits patients.
Therapists offer practical insight.
Collaboration improves judgement.
Shared learning strengthens care.
Understanding lived experience matters.
Empathy improves communication.
Better relationships lead to better outcomes.
Overcompensation can cause new problems.
Doctors should watch for this.
Early advice prevents damage.
Posture, breaks, and pacing matter.
Doctors can guide simple habits.
Small changes protect health.
Work ability changes with age.
Doctors should help plan ahead.
This ensures long-term stability.
Time since injury is less important than function.
Doctors should assess ability, not dates.
This leads to safer decisions.
Work supports dignity and independence.
Health protects long-term earning ability.
Both must be balanced carefully.
At the heart of return-to-work is a person, not a file.
Listening, observing, and guiding with care makes the difference.
This is how return-to-work decisions truly serve everyone.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body