
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Phantom limb pain is one of the most confusing and distressing problems faced by people after amputation. The limb is gone, yet the pain feels real, sharp, and often unbearable. For many patients, this pain becomes the biggest barrier to sleep, rehabilitation, and prosthetic use. For doctors, it is a condition that sits between surgery, nerves, and the brain, and it demands careful planning both before and after the operation.
This guide is written for clinicians who want clear, practical protocols for preventing and managing phantom limb pain. The focus is simple: early preparation, thoughtful surgical and medical care, and structured follow-up reduce the severity and duration of phantom pain. When doctors act early and stay consistent, patients recover faster, trust the process, and return to function with less fear and frustration.
Phantom limb pain is pain felt in a limb that has been surgically removed. The pain may feel burning, stabbing, squeezing, or like electric shocks. Patients often describe it as coming from fingers or toes that no longer exist.
This pain is different from stump pain. It does not arise from the surgical wound or local tissue damage. It comes from changes in the nervous system that occur before and after amputation.
Understanding this difference helps doctors choose the right prevention and treatment strategies.
The brain has a fixed map of the body. When a limb is removed, this map does not disappear. Instead, it becomes confused due to sudden loss of signals.
Nerves that once carried normal messages may start sending pain signals. The brain interprets these signals as coming from the missing limb.
This process explains why phantom pain can begin immediately or appear weeks later.
Not all patients develop phantom limb pain. Some feel only mild sensations or none at all. This difference depends on nerve health, pain history, emotional state, and how the surgery and recovery are managed.
Patients with long-standing pain before amputation are at higher risk. Poor pain control around surgery also increases risk.
This means phantom pain is not random. It can be influenced by clinical care.
When phantom pain is not addressed early, it often becomes chronic. Chronic pain is harder to treat and affects sleep, mood, and rehab participation.
Patients with severe phantom pain delay prosthetic training or abandon it altogether. This leads to loss of mobility and independence.
Early action reduces long-term suffering and improves functional outcomes.
Phantom pain should not be seen as a rare post-op complication. It is part of the amputation process for many patients.
Treating it as a continuum encourages doctors to plan ahead instead of reacting later. This shift changes outcomes.
Prevention is always easier than treatment in pain management.
Surgeons, physicians, anesthetists, and rehab doctors all influence phantom pain outcomes. Each stage of care adds or reduces risk.
When care is fragmented, patients receive mixed messages and delayed treatment.
A unified protocol ensures consistency and better control.
Patients with severe limb pain before surgery have a higher chance of phantom pain after amputation. This includes ischemic pain, infection-related pain, or nerve injury.
Mental health also plays a role. Anxiety, depression, and fear amplify pain perception.
Doctors should identify these risks early and plan accordingly.
A simple pain score is not enough. Doctors should ask about pain type, duration, triggers, and response to medicines.
Neuropathic pain before surgery often predicts phantom pain later.
Detailed history helps tailor pain control strategies.
Patients who are informed cope better. Explaining phantom sensations before surgery reduces fear when they occur.
Counseling should be honest but reassuring. Patients should know that phantom pain is common and treatable.
This conversation builds trust and reduces anxiety.
Poorly controlled pain before surgery sensitizes the nervous system. This increases the chance of phantom pain after amputation.
Doctors should aim to reduce pain intensity before the operation whenever possible.
Even partial relief lowers risk.
Neuropathic pain medicines, when started early, may reduce nerve sensitization. These medicines work best when introduced gradually.
Doctors should avoid last-minute changes unless necessary. Stability before surgery supports better outcomes.
Medication plans should be individualized.
Planning anesthesia in advance matters. Regional blocks can reduce nerve input during surgery.
This reduces sudden nerve shock to the brain. Patients who receive good regional pain control often report less phantom pain later.
Coordination with anesthesia teams is essential.
Surgical technique matters. Excessive nerve traction or rough handling increases nerve irritation.
Clean nerve cuts and proper positioning reduce abnormal nerve firing.
Surgeons should treat nerve handling as a key pain prevention step.
Neuromas are tangled nerve endings that can cause severe pain. Surgical techniques that reduce neuroma risk help reduce phantom pain severity.
Careful nerve management during surgery protects long-term comfort.
This step is often underestimated but highly impactful.
Minimizing tissue damage reduces inflammation and pain signals. Cleaner surgery supports smoother neural recovery.
Shorter surgery time and careful closure also help.
Good surgery is good pain control.
The first days after amputation are critical for the nervous system. During this time, the brain is trying to adjust to the sudden loss of signals from the limb. If pain signals dominate this period, the brain learns pain as the new normal.
When pain is well controlled immediately after surgery, the brain receives calmer input. This reduces the chance that pain pathways become fixed and persistent.
Doctors should treat early post-op pain control as a preventive step, not just comfort care.
After surgery, patients may feel pain from the wound, deep aching, or sharp nerve-related sensations. At the same time, they may report feelings in the missing limb, such as tingling or pressure.
Doctors should explain this difference clearly. Surgical pain comes from healing tissues, while phantom sensations come from the nervous system adjusting.
Clear explanation prevents fear and helps patients report symptoms accurately.
Patients often worry when they feel pain in a limb that is no longer there. If unprepared, they may think something has gone wrong.
Doctors should normalize these sensations early. Explaining that phantom feelings are common reduces panic and stress.
Calm patients cope better, and reduced stress directly lowers pain intensity.
Phantom limb pain is complex. It involves nerves, the spinal cord, and the brain. Using a single drug rarely controls all aspects of this pain.
A multimodal approach targets pain from different angles. This often allows lower doses of each medicine, reducing side effects.
Doctors should think in terms of balance, not strength.
Medicines that calm overactive nerves play an important role early after surgery. They reduce abnormal firing before pain patterns settle in.
Starting these medicines early, rather than waiting for severe pain, leads to better results. Dose adjustments should be slow and guided by response.
Consistency matters more than rapid escalation.
Basic pain medicines still have value. When surgical pain is controlled, overall pain perception reduces.
However, over-reliance on strong painkillers can mask symptoms without addressing nerve pain. This may delay proper phantom pain management.
Doctors should review pain patterns daily and adjust treatment accordingly.
Phantom limb pain often starts subtly. Patients may describe odd sensations before clear pain begins.
Doctors should listen without dismissing these early reports. Early acknowledgment builds trust and allows early intervention.
Waiting for severe pain makes treatment harder.
Some patients feel pain at night, while others notice it during rest. Stress and fatigue often worsen symptoms.
Pain may come in waves rather than constant discomfort. These patterns offer clues about nervous system involvement.
Careful documentation helps track progression.
Not all pain after amputation is phantom pain. Infection, pressure, or neuroma pain can mimic it.
Doctors should examine the limb carefully before labeling pain as phantom. Treating the wrong cause delays relief.
Accurate diagnosis is the foundation of effective care.
After amputation, the brain loses normal sensory feedback. Gentle, controlled touch around the residual limb provides new, safe input.
This helps the brain reorganize without defaulting to pain. Early desensitization reduces fear of contact.
Doctors should encourage guided sensory exposure as soon as safe.
Poor positioning increases swelling and discomfort, which can worsen nerve sensitivity. Proper support and positioning reduce background pain.
Calm tissues send calmer signals to the brain. This indirectly reduces phantom pain intensity.
Simple nursing measures often have large effects.
Gentle movement improves circulation and reduces stiffness. It also gives the brain useful feedback from nearby muscles.
Movement should always respect surgical healing, but complete immobility increases pain risk.
Doctors should guide safe, early activity with the rehab team.
Fear heightens pain perception. When patients are afraid of pain, the brain becomes more alert to discomfort.
This creates a cycle where fear increases pain, and pain increases fear. Breaking this cycle early is crucial.
Doctors play a key role through reassurance and clear explanations.
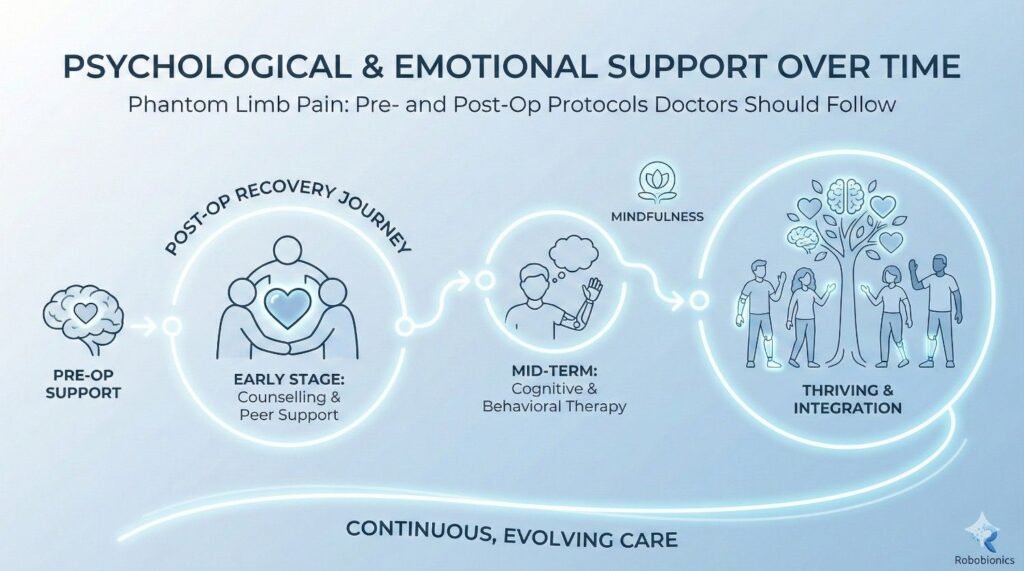
Amputation is a major life event. Grief, anger, and sadness are normal responses.
Unaddressed emotional distress often shows up as physical pain. A patient who feels unheard may report higher pain levels.
Simple empathy and validation reduce this burden.
If patients show extreme distress, panic, or withdrawal, early mental health input helps. This is not a failure of care but a strength.
Early support reduces long-term pain and improves rehab engagement.
Doctors should not hesitate to refer when needed.
As healing progresses, surgical pain should reduce steadily. When pain persists or changes in nature, phantom pain should be considered.
Burning, shooting, or electric sensations are key clues. Timing also matters, especially pain appearing after initial improvement.
Doctors should reassess pain type regularly.
Pain management should evolve with recovery. What worked in the first week may not be ideal in the third.
Gradual shifts from surgical pain control to nerve-focused strategies improve outcomes.
Static plans often fail in dynamic recovery phases.
Chronic phantom pain develops when early pain is poorly controlled or ignored. Early, active management reduces this risk significantly.
Doctors should aim to reduce pain intensity and frequency steadily, not just react to spikes.
Consistency and follow-up are essential.
For some patients, phantom limb pain does not fade after the early healing period. Instead, it becomes part of daily life, appearing during rest, stress, or sleep. This persistence happens when pain pathways in the brain and spinal cord remain active.
Once these pathways are established, the brain continues to expect pain signals from the missing limb. The pain becomes less about the surgery and more about learned nerve responses.
Doctors should explain this clearly so patients understand that persistence does not mean damage or failure.
Chronic phantom pain usually shows a pattern. It may appear at similar times each day or during emotional stress. The pain quality often stays neuropathic, with burning or sharp sensations.
Unlike surgical pain, it does not steadily improve on its own. Waiting for it to fade without intervention often leads to worsening intensity.
Early recognition allows timely change in treatment approach.
The goal of long-term care is not always complete pain removal. For many patients, reducing frequency, intensity, and emotional distress is a more realistic target.
Doctors should help patients measure success in function and comfort, not pain scores alone.
This perspective reduces frustration and improves adherence.
Rehabilitation is not only about strength and movement. It is also a form of pain therapy. Movement, balance, and coordination send new signals to the brain.
These signals help reorganize brain maps that were disrupted by amputation. Over time, this reduces phantom pain.
Doctors should encourage rehab even when pain is present, with proper guidance.
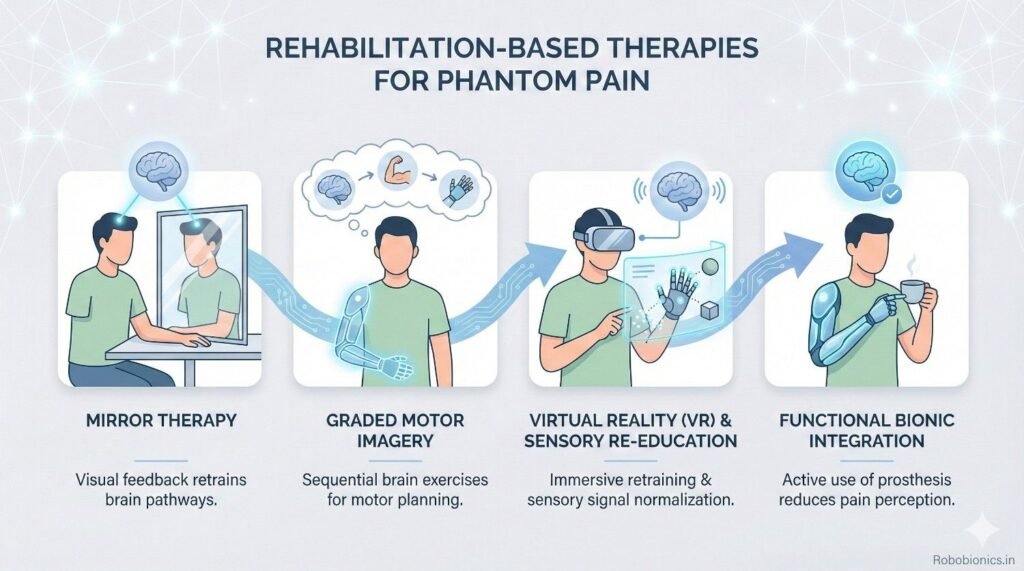
Mirror therapy uses visual input to trick the brain into seeing the missing limb move. This visual feedback can reduce pain by calming confused brain signals.
Some patients respond quickly, while others need weeks of practice. Consistency is more important than immediate results.
Doctors should present it as a tool, not a cure.
Graded motor imagery involves step-by-step mental and visual exercises that retrain the brain. It starts with imagining movement and progresses slowly.
This method reduces fear and overactivity in pain pathways. It is especially useful in patients with severe or long-standing pain.
Doctors should coordinate with trained therapists for best results.
Wearing a prosthesis provides the brain with new sensory and movement information. This input helps replace missing signals from the lost limb.
Many patients report reduced phantom pain once they start regular prosthetic use. The limb feels “occupied” rather than missing.
Doctors should encourage gradual, consistent use.
A poorly fitting socket increases pain and nerve irritation. This can worsen phantom pain instead of reducing it.
Comfortable, stable fit allows patients to focus on movement rather than discomfort. This supports positive brain adaptation.
Doctors should work closely with prosthetists to address fit issues early.
Starting prosthetic training when pain is completely absent is unrealistic. However, severe uncontrolled pain should be addressed first.
Doctors should aim for manageable pain levels before intensive training. This balance improves learning and reduces setbacks.
Flexibility in timing supports better outcomes.
Some patients require longer-term medication support. These medicines help quiet overactive nerve signals.
Doctors should review benefits regularly and avoid indefinite continuation without reassessment. Dose reduction may be possible as pain improves.
Clear follow-up plans prevent dependency and side effects.
Strong pain medicines may provide short-term relief but often fail in long-term phantom pain. They do not address the nerve-based cause.
Long-term use increases side effects and reduces quality of life. Doctors should use them cautiously.
Education helps patients understand why these medicines are limited.
Best results come from combining medication with rehab and psychological support. Each method supports the others.
Doctors should explain this combined approach clearly so patients do not expect pills alone to solve the problem.
Integrated care improves success rates.
Chronic pain and emotional health are closely linked. Anxiety, depression, and poor sleep increase pain sensitivity.
Patients may feel hopeless if pain persists despite treatment. This emotional weight often worsens symptoms.
Doctors should address emotional health as part of pain care.
Counseling helps patients develop coping skills and reduce fear of pain. Techniques that calm the mind reduce nerve overactivity.
Even brief supportive sessions can make a difference. Referral does not imply weakness.
Mental resilience supports physical recovery.
Phantom pain often reminds patients of loss. Addressing self-image and confidence helps reduce emotional distress.
Encouraging independence and social engagement improves overall well-being.
Doctors should look beyond pain to the whole person.
Phantom pain changes over time. Regular follow-up allows timely adjustments.
Doctors should ask open-ended questions rather than relying only on pain scores.
This approach uncovers hidden issues.
Patients should be encouraged to note when pain worsens. Triggers may include stress, poor sleep, or inactivity.
Identifying triggers allows targeted interventions.
Simple tracking empowers patients.
If pain remains severe despite standard care, referral to pain specialists is appropriate. Advanced therapies may be needed.
Early escalation prevents prolonged suffering.
Doctors should act proactively.
Patients with diabetes or vascular disease often have nerve damage even before amputation. This pre-existing nerve sensitivity increases the risk of severe phantom limb pain.
Poor blood flow and delayed healing also increase discomfort in the residual limb, which can worsen nerve signaling. Pain may feel more intense and last longer.
Doctors should plan more aggressive prevention and closer follow-up for these patients.
Traumatic amputations often involve sudden nerve injury and high emotional stress. The nervous system has little time to adapt before limb loss.
These patients may develop strong phantom sensations early. Pain may be linked with memory of the injury itself.
Early counseling and structured pain control are especially important in this group.
Children may struggle to describe phantom pain clearly. They may express it through behavior, sleep changes, or mood shifts.
Young adults may hide pain to appear strong or independent. This delays treatment.
Doctors should adapt communication style and involve caregivers appropriately.
Early phantom sensations are often mild and vague. Dismissing them as temporary can allow pain to become established.
Doctors should validate symptoms even when they seem minor.
Early response reduces long-term intensity.
While emotions influence pain, phantom limb pain has a strong biological basis. Labeling it as “in the mind” harms trust.
Patients need to feel believed and supported.
Balanced explanation improves cooperation.
Many clinicians wait too long to introduce therapies like mirror work or graded motor imagery. Delay reduces effectiveness.
These methods are safe and can begin early.
Doctors should not reserve them as last options.
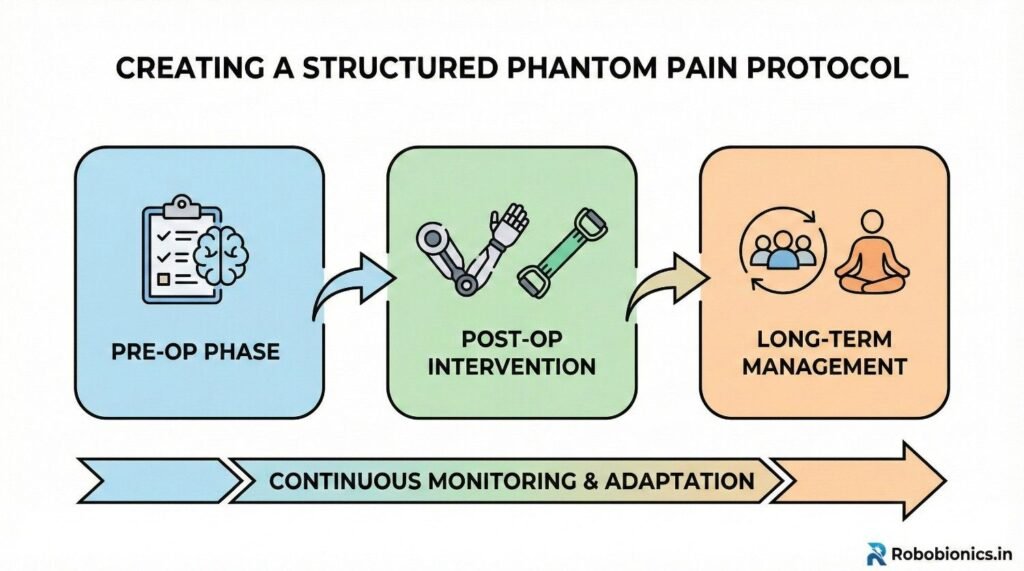
A simple checklist helps identify high-risk patients, review pain history, and plan anesthesia and counseling.
Standardization reduces variation in care.
Doctors can adapt checklists to their setting.
Daily pain review should include type, location, and triggers. This helps differentiate surgical and phantom pain.
Early adjustments improve control.
Consistency matters more than complexity.
Scheduled reviews at set intervals ensure pain is not ignored once wounds heal.
Clear referral pathways improve access to advanced care.
Structure supports continuity.
Patients should know that phantom feelings are common and not dangerous. This reduces fear.
Clear explanation improves reporting.
Education should be repeated.
Breathing exercises, gentle touch, and visualization help patients manage pain between visits.
Empowering patients reduces helplessness.
Simple tools are often effective.
Family members help observe patterns and encourage therapy adherence.
Education should include them whenever possible.
Shared understanding improves outcomes.
Improved sleep, better rehab participation, and prosthetic use reflect pain control success.
Pain reduction should support function.
Doctors should track these outcomes.
Patients who feel in control report better quality of life, even with some pain.
Confidence reduces pain focus.
Clinicians should encourage progress recognition.
The goal is a life that feels worth living, not zero pain.
This perspective guides realistic care.
Phantom limb pain is easier to prevent than to reverse. Early planning and consistent care reduce suffering.
Doctors who act early protect long-term outcomes.
Preparation matters.
No single clinician can manage phantom pain alone. Surgery, rehab, prosthetics, and mental health all play roles.
Coordination improves results.
Patients benefit from unity.
Mobility without comfort is not success. Phantom pain management restores dignity along with movement.
Thoughtful protocols change lives.
This is the true measure of good prosthetic care.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body