
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Prosthetic fitting is never just a technical step. It is a clinical decision that affects safety, recovery, and long-term quality of life. For clinicians, knowing when not to fit a prosthesis is just as important as knowing when to move forward. This is where a clear understanding of contraindications becomes essential.
This guide is written to help clinicians think clearly about absolute and relative contraindications to prosthetic fitting. It uses simple language, real clinical reasoning, and practical examples to support safer decisions and better patient outcomes.
The first duty of any clinician is to do no harm.
A prosthesis can help recovery, but in the wrong situation it can increase risk.
Contraindications exist to protect patients from avoidable injury and failure.
When fitting is done too early or without readiness, outcomes suffer.
Skin breaks down, pain increases, and confidence drops.
Clear contraindication assessment prevents these issues.
Many patients who abandon prostheses do so after a poor first experience.
Often, the real issue was not the device, but timing or readiness.
Contraindications help clinicians avoid setting patients up for failure.
A delayed but well-timed fitting is better than an early, harmful one.
This approach supports long-term acceptance and use.
Patience often leads to better results.
Clinicians are often under pressure from patients or families to proceed.
Contraindications provide a clinical framework to explain delays clearly.
They shift the discussion from opinion to patient safety.
Clear reasoning also protects clinicians professionally.
Decisions backed by sound contraindication logic are easier to defend.
This builds trust within teams and with patients.
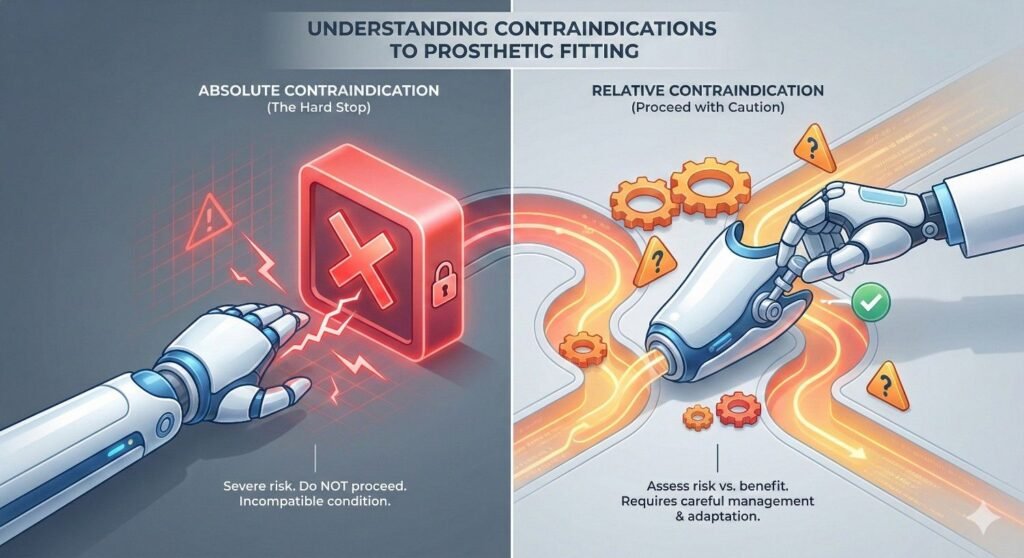
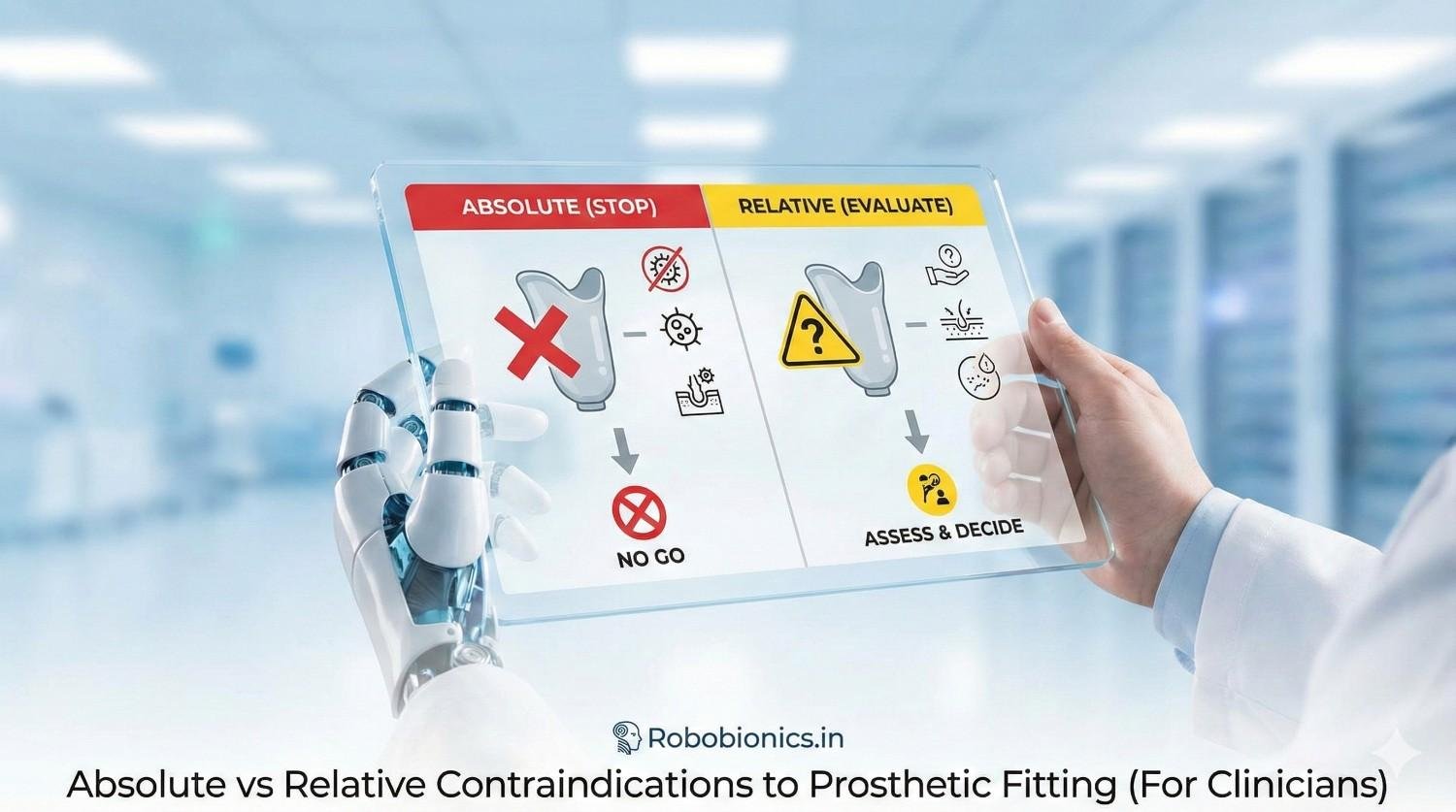
Absolute contraindications are conditions where prosthetic fitting should not proceed.
The risk of harm clearly outweighs any possible benefit.
In these cases, fitting must be delayed or avoided until the issue resolves.
These are usually medical or local limb issues.
They are not negotiable or preference-based.
Ignoring them often leads to serious complications.
Relative contraindications require clinical judgment.
They do not automatically block prosthetic fitting.
Instead, they signal higher risk that must be managed carefully.
In some cases, fitting may proceed with modifications or support.
In others, short-term delay may be safer.
The decision depends on the full patient context.
Confusing relative contraindications with absolute ones can deny care unnecessarily.
Ignoring relative risks can cause preventable failure.
The distinction helps clinicians choose the safest path forward.
Clear classification also improves team communication.
Everyone understands whether the goal is delay, modification, or avoidance.
This clarity reduces conflict and confusion.
Active infection at the stump is a clear absolute contraindication.
Fitting over infection increases spread, pain, and tissue damage.
It also compromises wound healing and socket tolerance.
Signs include discharge, redness, warmth, and systemic symptoms.
Even mild infection should be treated before fitting.
Prosthetic pressure worsens these conditions rapidly.
Clinicians should prioritize infection control first.
Prosthetic planning can happen in parallel without fitting.
This keeps patients informed without increasing risk.
Open wounds, dehisced scars, or unstable grafts cannot tolerate socket pressure.
Fitting too early often leads to wound breakdown.
This can delay recovery by weeks or months.
Even small unhealed areas matter.
Socket forces are repeated and unforgiving.
Healing must be stable, not just improving.
Clinicians should wait for consistent epithelialization.
Protective dressings alone are not enough.
Stable healing is the minimum requirement.
Poor blood flow prevents tissue from tolerating pressure and shear.
In ischemic limbs, even mild socket contact can cause breakdown.
Pain and ulceration are common outcomes.
Signs include rest pain, color changes, and poor capillary refill.
Vascular evaluation should guide timing decisions.
Revascularization may be needed before prosthetic fitting.
Proceeding without addressing perfusion risks limb loss progression.
In these cases, fitting is unsafe.
Delay protects remaining tissue.
Patients with unstable heart disease are at high risk during prosthetic training.
Increased energy demand can trigger cardiac events.
Safety must take priority over mobility goals.
Conditions such as uncontrolled heart failure or recent infarction require stabilization.
Training intensity alone can be dangerous.
Prosthetic fitting should wait until clearance is given.
Clinicians should coordinate with cardiology.
Gradual rehab planning can happen without fitting.
Medical stability comes first.
Prosthetic ambulation increases oxygen demand.
Patients with severe uncontrolled lung disease may not tolerate training.
Breathlessness and fatigue limit safe use.
If basic activities cause significant distress, fitting should be delayed.
Respiratory optimization improves later success.
Ignoring this risk leads to rapid abandonment.
Clinicians should reassess after pulmonary stabilization.
This protects patients and improves outcomes.
Timing matters more than speed.
Acute illness such as sepsis or metabolic instability is an absolute contraindication.
The body needs energy to heal and recover.
Prosthetic fitting adds unnecessary stress.
During acute illness, focus should remain on recovery.
Rehabilitation planning can resume once stable.
Early fitting in this phase offers no benefit.
Clear communication helps manage expectations.
Delay does not mean denial.
It means safer care.
Severe cognitive impairment limits safe prosthetic use.
Patients may not understand instructions or danger.
This increases fall and injury risk.
In such cases, fitting may do more harm than good.
Simpler mobility aids may be safer.
The goal shifts to comfort and transfers.
Clinicians should involve caregivers in decision-making.
Ethical clarity is essential.
Safety must guide the choice.
Uncontrolled psychosis, severe agitation, or active suicidal behavior are contraindications.
Prosthetic fitting requires focus, learning, and emotional regulation.
Instability undermines safe training.
These conditions may be temporary.
Mental health treatment can change readiness.
Reassessment after stabilization is appropriate.
Proceeding too early risks injury and distress.
Delay supports better long-term success.
Mental health is part of medical readiness.
Some patients repeatedly use devices unsafely despite education.
This may include refusal of precautions or reckless behavior.
When risk remains high, fitting may be unsafe.
This decision should never be punitive.
It should be based on repeated documented risk.
Alternative mobility options should be offered.
Clinicians should document clearly and compassionately.
Safety remains the guiding principle.
Care continues, even if fitting does not.
Fragile skin increases the risk of breakdown but does not always prevent fitting.
Elderly patients or those with long-term illness often fall into this group.
Careful socket design and monitoring can help.
Relative risk can be managed with shorter wear times.
Frequent skin checks are essential.
Education becomes a key part of care.
Clinicians should weigh benefit versus monitoring burden.
Support systems matter greatly here.
Decision-making should be individualized.
Large volume changes make socket fit unstable.
This increases friction and pressure points.
However, volume change is often temporary.
Temporary or preparatory prostheses may be suitable.
Compression and limb shaping can help.
Time often resolves this issue.
Clinicians should not see volume change as permanent exclusion.
It signals the need for staged care.
Planning prevents frustration.
Joint contractures limit prosthetic alignment and function.
Mild to moderate contractures may still allow fitting.
Severe ones may require correction first.
Physiotherapy can improve range over time.
Sometimes fitting encourages movement.
The decision depends on severity and goals.
Clinicians should coordinate closely with therapists.
Joint range should be reassessed regularly.
Flexibility improves options.
Diabetes, hypertension, or kidney disease increase risk when uncontrolled.
However, many patients improve with medical optimization.
Fitting may proceed cautiously in stable phases.
Relative contraindication means closer monitoring is needed.
Goals may need adjustment.
Education is critical.
Clinicians should avoid blanket exclusion.
Stability, not diagnosis, guides readiness.
Regular review supports safer use.
Deconditioned patients tire quickly and struggle with training.
This does not always mean prosthetics are inappropriate.
It means expectations must be realistic.
Short training sessions and simple devices may help.
Rehab can improve tolerance over time.
Progress should be slow and supported.
Clinicians should reassess endurance regularly.
Improvements can change indications.
Deconditioning is often reversible.
Higher body weight increases socket pressure and energy demand.
This raises risk but does not always prevent fitting.
Device selection and training pace matter.
Weight management support improves outcomes.
Honest discussion about effort is essential.
Safety should guide progression.
Clinicians should avoid stigma in these conversations.
Focus on function and support.
Respect improves engagement.
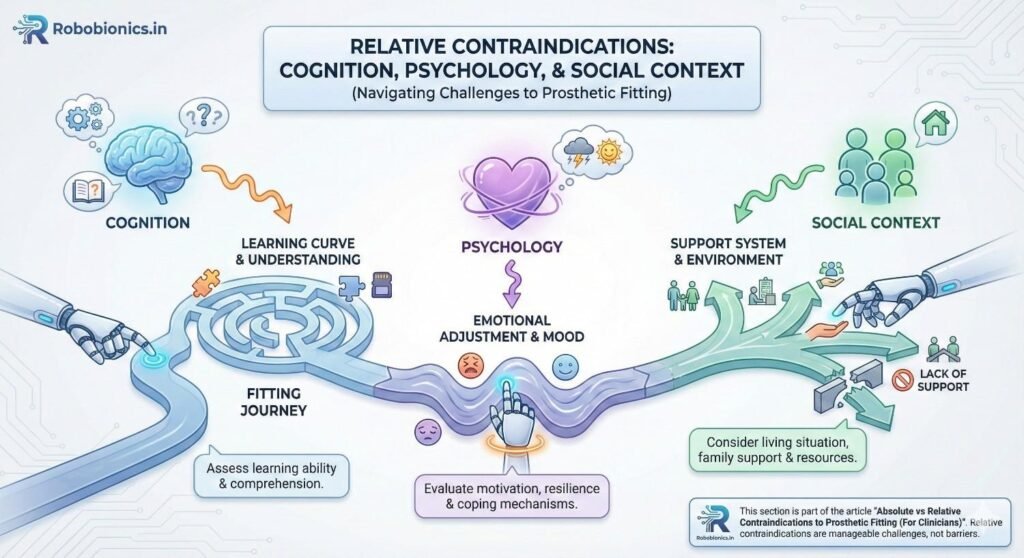
Patients with mild or moderate cognitive impairment may still benefit from prosthetic fitting, but they require careful assessment and structured support. The key question is not whether the patient has a diagnosis, but whether they can follow basic safety instructions, learn routines, and recognize discomfort or danger. When these abilities are present, prosthetic fitting can proceed with added supervision and simplified goals.
In such cases, clinicians should involve caregivers early and clearly define roles in daily supervision and skin checks. Training sessions may need to be shorter and repeated more often, with emphasis on consistency rather than speed. When support systems are reliable, cognitive limits become a manageable risk rather than a barrier.
Emotional distress is common after limb loss and should not automatically delay prosthetic fitting. However, untreated or severe symptoms can affect motivation, learning, and persistence, which in turn influence outcomes. Clinicians must judge whether emotional state is likely to interfere with safe use or whether prosthetic fitting may actually support recovery.
When distress is moderate and the patient remains engaged, prosthetic fitting can proceed alongside counseling or mental health support. When symptoms dominate daily function or lead to withdrawal, delay may be appropriate until stabilization occurs. The goal is not to wait for perfect emotional health, but to ensure enough stability to benefit from training.
Some patients believe a prosthesis will fully restore normal function with little effort, while others underestimate its value and see it as pointless. Both extremes can reduce success if not addressed early. Unrealistic expectations are a relative contraindication because they raise the risk of disappointment and abandonment rather than direct harm.
Clinicians should spend time aligning expectations with reality through clear, simple explanations and examples. When expectations can be adjusted through education and shared goal setting, fitting can move forward safely. If insight remains poor despite repeated counseling, delaying fitting may protect both patient and team from frustration.
Lack of social support increases risk, especially in the early fitting phase when monitoring and encouragement are important. Patients living alone or without family help may struggle with skin care, device management, and follow-up. This does not automatically rule out prosthetic fitting, but it changes how care must be planned.
In these situations, clinicians should explore community resources, home health support, or extended inpatient training where possible. If no support can be arranged and risk remains high, delay may be the safer choice until systems are in place. Social context is a clinical factor, not a personal failing.
Many absolute contraindications are not permanent. Infections resolve, wounds heal, and medical conditions stabilize with treatment. Clinicians should communicate clearly that delay is often temporary and part of a planned pathway, not a dead end.
During this waiting period, early prosthetic education, limb shaping, and therapy can continue so that fitting can begin quickly once readiness is achieved. This approach keeps patients engaged and reduces frustration. Time is used productively rather than wasted.
Relative contraindications such as poor endurance, weakness, or joint stiffness often improve with focused rehabilitation. What is unsafe today may be appropriate in a few weeks or months. Regular reassessment is essential to avoid outdated decisions.
Clinicians should set clear milestones that signal when reassessment will occur. This gives patients tangible goals and maintains motivation. Dynamic decision-making leads to better long-term outcomes.
A patient’s goals may evolve as recovery progresses. Early on, comfort and transfers may matter most, while later the focus may shift to independence or work. Contraindications should be reviewed in light of these changing goals.
Clinicians should remain open to revisiting decisions rather than assuming that an early judgment applies forever. Flexibility respects patient autonomy and reflects real life recovery patterns.
When relative contraindications are present, the prosthetic plan should be adapted to reduce risk. This may include simpler devices, limited initial wear time, or staged progression toward full use. The goal is to match challenge level with readiness.
Clinicians should document these modifications clearly so all team members understand the intent. This prevents misalignment and unsafe escalation. Careful planning allows fitting to proceed while protecting the patient.
Higher risk situations require closer follow-up. Early and frequent reviews allow clinicians to identify skin issues, pain, or unsafe use before they escalate. This is especially important in patients with sensory loss or limited insight.
Clear instructions on when and how to seek help should be given in simple language. Patients and caregivers should feel encouraged, not blamed, when concerns arise. Monitoring is a support tool, not a test.
When contraindications are relative rather than absolute, communication between doctors, prosthetists, and therapists becomes even more important. Regular updates ensure that emerging issues are addressed promptly and consistently.
Clinicians should promote a shared understanding of risk and goals rather than isolated decisions. Team-based awareness reduces errors and improves confidence across disciplines.
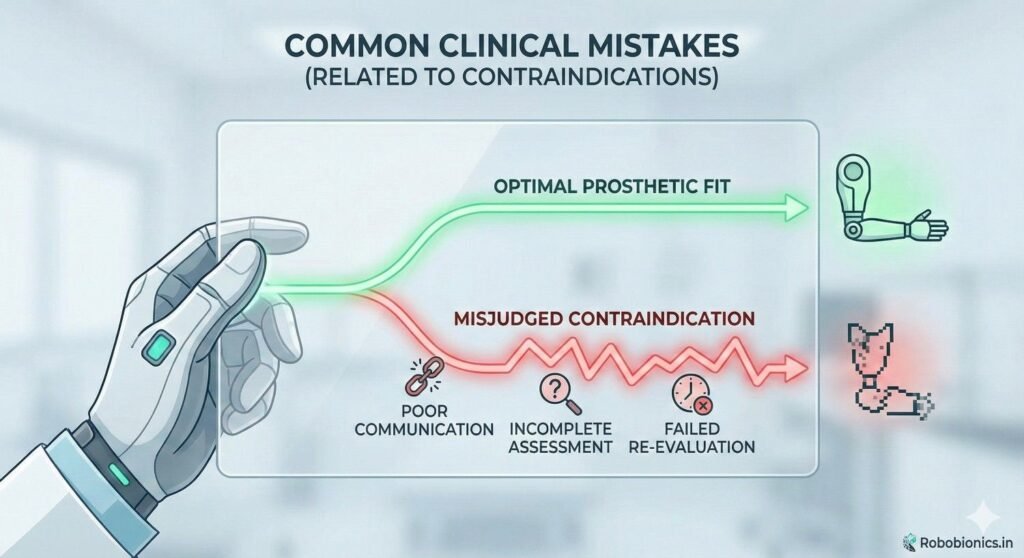
One common mistake is excluding patients unnecessarily by treating relative risks as permanent blocks. This often happens when time or resources are limited, leading to overly cautious decisions.
While safety must always come first, denying prosthetic care without reassessment can reduce quality of life and long-term function. Clinicians should strive for balanced judgment rather than default refusal.
The opposite mistake is ignoring early signs that fitting is not going well, such as repeated skin issues, fear, or declining use. These are often signals that a relative contraindication has become more significant.
Prompt reassessment and adjustment protect patients and preserve trust. Delay at this stage is often safer than persistence without change.
When contraindications are not clearly documented, confusion and conflict can arise later. Patients, families, and team members may misunderstand why decisions were made.
Clear documentation of clinical reasoning, risks, and plans for reassessment protects both patients and clinicians. It also supports continuity of care across settings.
Delaying prosthetic fitting can feel devastating to patients. Clinicians must explain that delay is a safety decision, not a rejection. Language should focus on preparation and protection rather than denial.
When patients understand the reason for delay and see a clear plan forward, trust is preserved. Hope is maintained through honesty and clarity.
In relative contraindication scenarios, shared decision-making is essential. Patients should understand the risks, possible benefits, and alternatives in simple terms.
Clinicians should guide rather than dictate, while still setting boundaries around safety. Shared decisions lead to better engagement and adherence.
In rare cases where prosthetic fitting is not appropriate, clinicians must approach the conversation with empathy and respect. Alternative mobility or assistive options should be discussed in detail.
The goal is to preserve dignity and independence in other ways. Good care continues even when prosthetic fitting does not.
At RoboBionics, we work closely with clinicians to understand both the possibilities and limits of prosthetic fitting. Our designs account for real-world constraints such as skin tolerance, endurance, and access to follow-up.
We believe that acknowledging contraindications openly leads to better device selection and safer outcomes. Technology should adapt to patients, not the other way around.
We support staged prosthetic approaches that allow fitting to begin safely even when risks are present. Temporary devices, modular designs, and training support help clinicians manage relative contraindications with confidence.
Our goal is to work alongside medical teams, not replace clinical judgment. Collaboration leads to sustainable success.
Affordability reduces pressure to rush fitting or overpromise outcomes. When care is accessible, clinicians can focus on timing and readiness rather than cost urgency.
This balance supports ethical decision-making and long-term patient trust.
One of the most important ideas for clinicians to hold is that contraindications change with time. What is unsafe today may become safe after healing, therapy, or medical optimization. Treating contraindications as fixed labels can unintentionally block recovery.
Regular reassessment should be built into care plans. This keeps decisions current and aligned with the patient’s real condition. It also shows patients that the team is watching progress closely and not making permanent judgments too early.
Dynamic thinking leads to better long-term outcomes.
Rather than giving vague advice like “come back later,” clinicians should set clear checkpoints. These may be based on wound healing, infection resolution, improved endurance, or better mental health stability.
Clear checkpoints give patients something concrete to work toward. They also make it easier for teams to coordinate and plan next steps. Structure reduces anxiety and improves adherence.
Reassessment should be intentional, not incidental.
When contraindications are not revisited, patients may drift into long periods without progress. This often happens when responsibility for follow-up is unclear or when teams assume someone else is reassessing readiness.
Clinicians should take ownership of follow-up decisions or clearly hand them over. Clear responsibility prevents patients from being lost between services.
Good systems protect patients from silence.
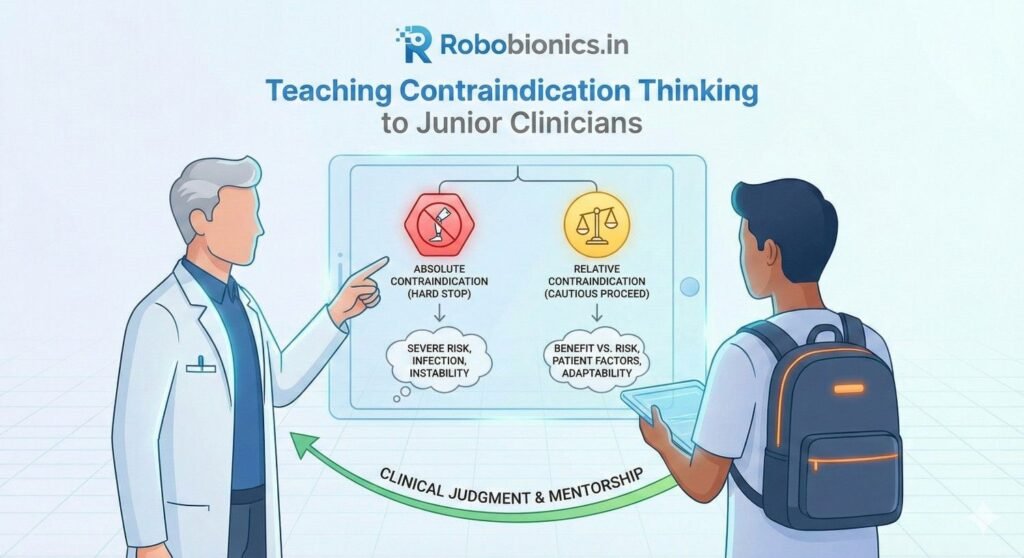
Junior clinicians often fear making the wrong decision and may avoid prosthetic referrals altogether. Teaching contraindications properly helps them understand risk without becoming overly cautious.
Training should focus on reasoning rather than rules alone. Explaining why a condition is a contraindication helps clinicians apply the concept flexibly and safely.
Confidence grows from understanding, not avoidance.
Real patient cases are the best way to teach contraindications. Discussing what went wrong in failed fittings or what improved after waiting builds practical insight.
These discussions should be open and non-punitive. Learning comes from reflection, not blame.
Shared learning strengthens teams.
Contraindication assessment improves when doctors learn alongside prosthetists and therapists. Each discipline sees different risks and signals.
Joint discussions build shared language and reduce miscommunication. They also help junior clinicians see prosthetic fitting as a team decision rather than a solo call.
Team learning leads to safer care.
When prosthetic fitting is not advised, clinicians must ensure that alternative mobility solutions are strong and supported. This may include wheelchairs, walkers, or environmental modifications.
These options should not be presented as lesser care. They are valid clinical solutions when prosthetic risk is too high.
Quality of life remains the goal.
Patients may feel discouraged when prosthetic fitting is delayed or avoided. Clinicians should actively address concerns about dependence and identity.
Clear explanations, respectful language, and practical alternatives help preserve dignity. Independence can take many forms.
Good care adapts, not withdraws.
Even when fitting is not appropriate now, clinicians should keep the door open for future reassessment. Circumstances change, and hope should remain grounded but alive.
Patients should know that care continues and options will be revisited. This reassurance matters deeply.
Hope must be honest, not absent.

Absolute and relative contraindications exist to guide safer care, not to block progress. When understood clearly, they help clinicians choose the right timing, the right approach, and the right level of support.
Absolute contraindications demand delay or avoidance to prevent harm. Relative contraindications invite careful judgment, modification, and monitoring. Both require thought, not reflex.
Clarity protects patients and clinicians alike.
No guideline replaces clinical judgment. Contraindications must always be interpreted in the context of the whole person, not just the limb or diagnosis.
Good judgment balances safety with opportunity. It avoids rushing but also avoids unnecessary denial of care.
This balance is the heart of good prosthetic medicine.
Safe prosthetic fitting depends on collaboration between doctors, prosthetists, therapists, patients, and caregivers. Contraindication decisions are strongest when shared and communicated clearly.
Open dialogue prevents errors and builds trust. Patients benefit most when teams move together.
Team-based care is safer care.
At RoboBionics, we see contraindications as an essential part of responsible prosthetic care. Our work with clinicians across India has shown that the best outcomes come when timing, readiness, and support are respected.
By designing affordable, flexible prosthetic solutions and supporting staged care pathways, we aim to help clinicians manage relative risks without pressure to rush. Our focus is on long-term success, not short-term fitting.
When clinical judgment and thoughtful technology work together, patients regain function with safety and dignity.
Knowing when not to fit a prosthesis is a sign of strong clinical care, not hesitation. Contraindications, when used well, protect patients, guide teams, and improve long-term outcomes.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body