
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Blood clots and delayed movement are silent barriers to prosthetic success. Many patients recover from surgery but struggle later because their body was not protected and activated early. Deep vein thrombosis, or DVT, and long periods of bed rest can quietly steal strength, confidence, and readiness for a prosthetic limb.
This article explains how DVT prevention and early mobility work together to prepare patients for successful prosthetic use. It focuses on clear actions that doctors, care teams, and patients can take before and after surgery to protect healing, restore movement, and keep the path to a prosthesis open.
Deep vein thrombosis often develops without clear warning signs, especially in patients who have undergone major surgery like amputation. Many patients do not feel pain or swelling in the early stages, which makes the condition easy to miss. By the time symptoms appear, the clot may already be large or may have moved to the lungs, creating a life-threatening situation.
For patients preparing for prosthetic use, this hidden danger has lasting consequences. A DVT diagnosis often leads to extended bed rest, strict movement limits, and long courses of blood-thinning medicines. These steps, while necessary, delay recovery and reduce the body’s readiness for prosthetic training.
Prosthetic success depends on movement, strength, and balance. When DVT occurs, these foundations are disrupted. Patients are often told to limit activity, which leads to muscle weakness and joint stiffness. Even short periods of immobility can slow progress in a body that is already adapting to limb loss.
Delayed movement also affects confidence. Patients may begin to fear walking or standing, even after the clot is treated. This fear becomes a mental barrier that can be harder to overcome than physical weakness.
Preventing DVT keeps the recovery journey moving forward. When blood flow is protected and movement continues safely, patients retain strength and confidence. This allows rehab to start on time and keeps prosthetic planning on track.
In prosthetic care, prevention is not just about avoiding harm. It is about protecting opportunity. A patient free from DVT is a patient who can continue preparing for independence.
Amputation surgery places heavy stress on the body. Blood vessels are disrupted, inflammation increases, and natural movement is reduced. These changes slow blood flow, especially in the deep veins of the legs, creating ideal conditions for clot formation.
Many amputation patients already have poor circulation due to diabetes or vascular disease. When surgery is added to this background, the risk multiplies. This is why amputation patients must always be treated as high-risk for DVT.
After surgery, patients often remain in bed due to pain, weakness, or fear. While rest is important, too much rest allows blood to pool in the veins. This pooling is one of the main causes of clot formation.
Even small movements, such as ankle pumps or sitting upright, help blood flow. When movement is delayed for days, the risk of DVT rises sharply and silently.
Conditions like obesity, heart disease, smoking, and advanced age further slow circulation and weaken the body’s ability to break down clots. Many patients have more than one of these risks.
Without careful planning, these factors combine and increase the chance of serious complications that delay or prevent prosthetic use.
DVT prevention must begin before surgery. Every patient should be assessed for clot risk using medical history, age, weight, and mobility level. This assessment should guide the prevention plan.
A clear risk profile allows the care team to act early instead of reacting later.
Blood-thinning medicines help reduce clot formation when used correctly. The dose and timing must be carefully selected to prevent clots without causing bleeding problems.
Clear communication about why and how these medicines are used improves patient trust and compliance.
Compression stockings and pneumatic compression devices support blood flow when movement is limited. These tools are effective only when used regularly and correctly.
Patients and staff must understand their purpose, not treat them as optional equipment.
Movement activates muscles that push blood through veins toward the heart. This natural pump reduces clot risk more effectively than any single medicine.
Early movement should be seen as a core part of treatment, not an extra activity added later.
Many patients are afraid to move after surgery. They worry about pain, falling, or damaging the wound. Without reassurance, this fear keeps them still.
Clear guidance from the care team helps patients understand that safe movement protects healing rather than harming it.
Early movement supports strength, balance, breathing, and posture. These elements are essential for future prosthetic control.
Movement builds the physical and mental base needed for learning to walk again.
Movement should begin as soon as the patient is stable. This may start with breathing exercises, leg movements in bed, or sitting upright.
Each step prepares the body for the next level of activity.
Mobility should increase slowly and safely. Sudden effort can increase pain or fear. A step-by-step plan helps patients trust the process.
Consistency matters more than speed.
Patients feel more confident when they know what is expected each day. Simple goals such as sitting up twice a day or standing with support give direction.
Clear goals turn recovery into a structured journey.
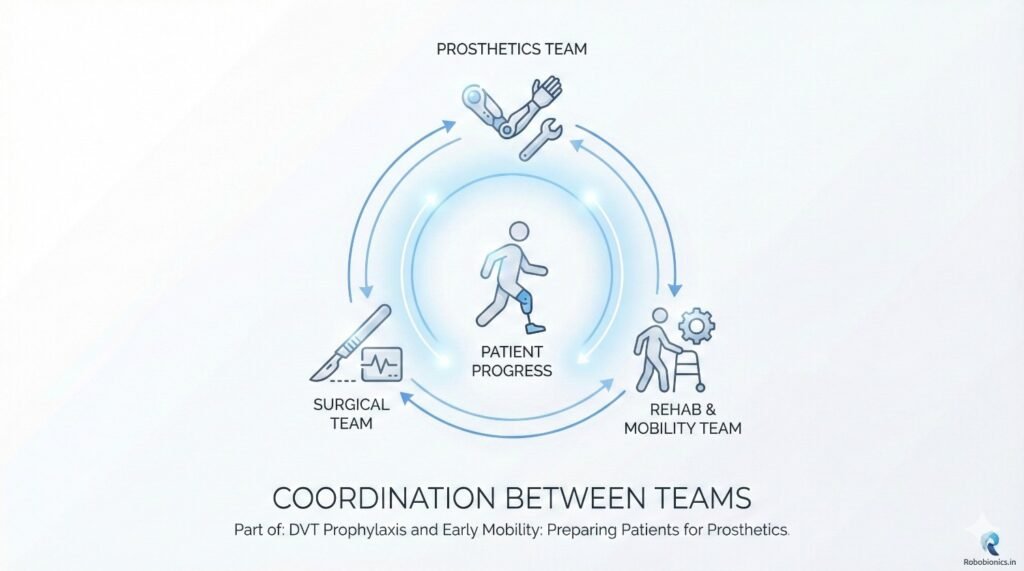
Doctors and surgeons must agree on when and how mobility should begin. Mixed messages confuse patients and delay progress.
Unified plans improve safety and trust.
Nurses and therapists are key drivers of early mobility. Their daily presence allows encouragement, correction, and reassurance.
Their role directly affects patient confidence.
Prosthetists benefit when patients remain strong and mobile. Early communication helps align rehab goals with future prosthetic needs.
Early planning reduces delays later.
Patients should understand that clots form when blood stops moving. Simple explanations help them see why movement matters.
Understanding leads to cooperation.
Patients need clear guidance on how to move safely without harming the wound. This includes posture, breathing, and rest periods.
Safety builds confidence.
When patients see movement as part of treatment, not a test, they engage more fully. Participation speeds recovery.
Active patients adapt better.
Muscles lose strength quickly during bed rest. Weak muscles make prosthetic control harder and slower to learn.
Early strength protects future function.
Lack of movement leads to stiff joints and pain. These limit walking ability and prosthetic comfort.
Movement preserves freedom.
Delayed mobility affects mental health. Patients may feel helpless or discouraged.
Early progress builds belief.
Older patients may fear movement more. Gentle support and reassurance help them stay active.
Confidence improves safety.
These patients need careful monitoring, but movement remains important. Avoiding movement often causes more harm than benefit.
Balance is key.
Emergency patients often miss early planning. Rapid coordination helps reduce risk.
Late action still matters.
Movement should be treated like medicine. Daily focus improves results.
Priority shapes behavior.
Tracking progress helps teams identify barriers and adjust plans. Awareness improves outcomes.
Measurement supports care.
Recognizing small progress builds motivation. Positive reinforcement encourages effort.
Success grows from encouragement.
When DVT is prevented and early movement is encouraged, the body stays active during a very sensitive phase of recovery. Muscles above the amputation level remain stronger, and core balance is better preserved. This strength becomes the base for prosthetic training.
Patients who maintain strength early find it easier to learn weight shifting, standing balance, and walking later. They spend less time relearning basic movements and more time improving function.
Early mobility keeps joints flexible and reduces stiffness. Hips, knees, and the lower back all play a major role in prosthetic walking. When these joints remain mobile, prosthetic alignment and training become smoother.
Good balance developed early also lowers fall risk during prosthetic trials. Patients feel safer and are more willing to practice.
Patients who move early and avoid DVT often reach prosthetic fitting sooner. Their residual limb shape stabilizes faster, swelling reduces steadily, and skin quality improves.
Early fitting keeps motivation high and prevents long gaps between surgery and functional recovery.
After limb loss, many patients feel they have lost control over their body and life. Early movement helps restore this sense of control. Even small actions like sitting up or standing supported can change how patients see themselves.
This sense of control improves cooperation with therapy and long-term care.
Fear often grows when the body stays still for too long. Patients begin to doubt their strength and safety. Early guided movement replaces fear with experience.
When patients see that movement is possible and safe, confidence grows naturally.
Small progress early builds hope. Standing for the first time or taking assisted steps creates belief. This belief fuels effort during prosthetic training.
Motivation built early often lasts through difficult rehab phases.
Hospitals that follow clear DVT prevention and mobility protocols often see fewer complications. Shorter hospital stays, fewer readmissions, and smoother rehab are common results.
These outcomes benefit both patients and healthcare systems.
Patients who avoid DVT and stay mobile are more likely to use their prosthesis daily. They report less pain, better balance, and higher confidence.
Prosthetic use depends on preparation, not just device quality.
When patients regain independence faster, the need for long-term care reduces. Families experience less stress, and patients return to work or daily roles sooner.
Early care choices shape long-term outcomes.
Physicians play a key role in shaping patient behavior. When doctors clearly state that movement is part of treatment, patients take it seriously.
Clear expectations reduce hesitation and confusion.
Not all patients progress at the same pace. Physicians must review mobility and DVT prevention plans regularly and adjust as needed.
Flexibility supports safety.
Consistency matters more than intensity. Physicians should reinforce steady daily movement rather than rare big efforts.
Regular activity builds lasting strength.
Patients should know that early movement and clot prevention are steps toward walking again. This connection increases cooperation.
Purpose improves effort.
Care teams should repeat this message during rounds, therapy, and discharge planning. Repetition builds understanding.
Understanding builds commitment.
When patients understand prosthetic goals early, they mentally prepare for the work ahead. This readiness improves training outcomes.
Preparation shapes success.
DVT risk does not end at discharge. Clear home mobility plans reduce risk. Patients should know how much to move and when to rest.
Guidance protects recovery.
Patients must know when and where to follow up. Delayed review increases risk of missed clots or reduced movement.
Access improves safety.
Family members often influence patient movement at home. Educating them prevents overprotection that limits mobility.
Support should encourage, not restrict.
Extended bed rest is one of the biggest barriers to prosthetic readiness. Rest should be balanced with movement.
Too much rest weakens recovery.
Restricting movement out of fear often causes more harm than benefit. Guided movement is safer than avoidance.
Confidence grows with action.
Conflicting advice delays mobility. Clear and shared plans prevent confusion.
Clarity supports progress.
Most DVT cases can be prevented with proper care. Allowing preventable harm affects patient trust and outcomes.
Prevention is a duty.
Every patient deserves the same prevention and mobility care, regardless of background.
Fair care builds better systems.
Responsibility does not end at hospital discharge. Long-term readiness depends on early actions.
Care must be continuous.
Movement after amputation is a skill that improves with practice. Early teaching builds this skill gradually.
Skills improve with repetition.
Patients should learn to notice swelling, pain, or breath changes. Early reporting protects safety.
Awareness supports prevention.
Active patients adapt better to prosthetic life. Early habits shape long-term behavior.
Habits build independence.
When DVT develops, physical therapy is often paused or reduced. Doctors may restrict movement to avoid clot travel, even when the patient feels ready. This pause breaks the natural recovery rhythm.
For amputation patients, delayed therapy means lost time during the most important recovery window. Muscles weaken faster during this phase, and restarting therapy later takes more effort.
The early weeks after surgery are when the brain adapts best to body changes. Patients learn balance, posture, and safe movement patterns during this phase. DVT interrupts this learning process.
When therapy restarts late, patients often struggle more because the body and mind are no longer in sync.
Patients who experience DVT usually need longer rehab programs. What could have been achieved in weeks may take months. This increases cost, fatigue, and frustration.
Prevention shortens the road back to function.
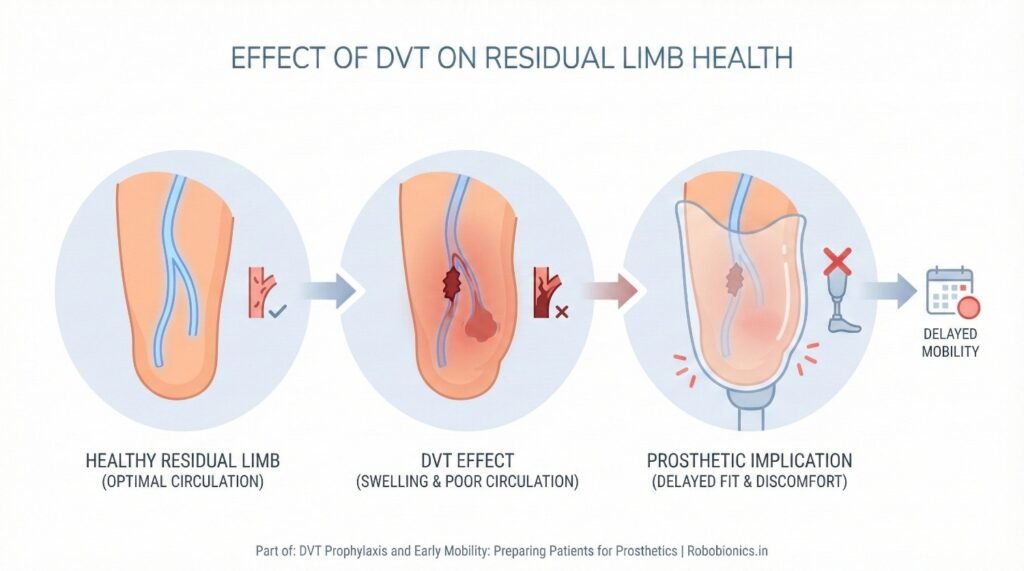
DVT often causes swelling in the limb, which may last even after treatment. This swelling makes the residual limb sensitive and unstable in shape.
A swollen limb cannot tolerate prosthetic pressure well, leading to discomfort and fitting delays.
Blood clots affect blood return from the limb. Poor circulation weakens skin and slows repair. Even small pressure points can turn into wounds.
Healthy blood flow is critical for strong prosthetic skin.
Residual limb shape must remain stable for a good prosthetic fit. DVT-related swelling and tissue changes often delay this stability.
Unstable shape leads to repeated adjustments and poor comfort.
Balance is not only about strength. It depends on early exposure to standing and weight shifting. DVT often delays these activities.
Patients who stand early regain balance faster and with less fear.
Standing for the first time after amputation is a major mental step. When this moment is delayed, fear often grows.
Early safe standing builds trust in the body.
Patients who regain balance early have fewer falls during prosthetic training. This improves safety and confidence.
Balance learned early stays longer.
Early movement improves breathing and heart function. Prolonged bed rest reduces lung capacity and increases strain on the heart.
Healthy heart and lungs support longer prosthetic training sessions.
Patients who move early experience less fatigue later. Their endurance remains higher, making therapy more effective.
Energy supports progress.
Good circulation improves healing across the body. This speeds up recovery beyond just the surgical site.
Whole-body health supports limb recovery.
Nurses spend the most time with patients. Their encouragement often determines whether patients move or stay in bed.
Small prompts from nurses create big behavior changes.
When nurses guide posture, breathing, and pacing, patients move more safely. This reduces fear and injury risk.
Safety builds trust.
Nurses often notice swelling, pain, or breathing changes first. Early detection of DVT signs saves lives and recovery time.
Observation is prevention.
Patients who move early begin to see themselves as recovering, not disabled. This identity shift affects effort and attitude.
Mindset shapes outcomes.
Long bed rest can make patients feel permanently unwell. Early mobility prevents this mental trap.
Movement restores normalcy.
Daily movement routines build discipline that carries into prosthetic training.
Routine creates progress.
Families often try to protect patients by limiting movement. While well-meaning, this increases DVT risk.
Education helps families support safely.
When families understand that movement prevents clots and speeds prosthetic readiness, they encourage activity instead of fear.
Knowledge changes behavior.
Simple changes at home can support safe movement. Planning early reduces setbacks.
Preparation supports recovery.
Patients who stay active early tend to remain active long term. This leads to better prosthetic use and independence.
Early habits last.
Stronger, more confident patients rely less on caregivers. This improves dignity and family balance.
Independence restores self-worth.
Patients who recover faster return to social roles and work sooner. This improves mental health and financial stability.
Function supports life quality.
After surgery, it is common to restrict movement out of caution. However, blanket restrictions often cause more harm than benefit. Not every patient needs the same limits, and excessive restriction increases DVT risk and slows recovery.
Clinical decisions around mobility should be personalized. When movement is limited without clear reason, the body pays the price through weakness and fear.
Safety is important, but safety does not mean stillness. With proper support, monitoring, and guidance, most patients can begin some level of movement early. The goal is not speed, but safe progress.
Physicians should guide teams to allow movement within clear limits rather than avoiding it altogether.
Mobility needs change quickly after surgery. Orders written once and not reviewed can delay recovery. Daily review ensures patients are not held back longer than needed.
Timely updates protect both safety and progress.
Pain is one of the biggest reasons patients avoid movement. When pain is poorly controlled, patients tense their body and resist therapy. This increases clot risk and stiffness.
Effective pain control supports movement and confidence.
Pain medicine should be planned to support therapy sessions and mobility times. Proper timing allows patients to move when pain is lowest.
Movement becomes possible when pain is managed well.
Too much pain medicine can cause drowsiness and fear of falling. This reduces mobility and increases clot risk. Balance is essential.
Clear pain plans support safe activity.
Deep breathing improves oxygen levels and supports circulation. Shallow breathing during bed rest reduces oxygen delivery and slows healing.
Breathing exercises should begin early.
Bed rest increases risk of lung infections and reduced lung function. These issues increase fatigue and limit rehab effort.
Healthy lungs support strong movement.
Prosthetic training requires stamina. Patients who protect lung health early perform better during long therapy sessions.
Breathing supports endurance.
Bones stay strong when they carry weight. Long periods without load weaken bones. Early standing and weight-bearing help protect bone health.
Strong bones support prosthetic safety.
Weak bones increase fracture risk during prosthetic training. Early movement reduces this risk.
Prevention protects confidence.
Bone health affects how forces travel through the limb during walking. Early care shapes long-term comfort.
Structure matters.
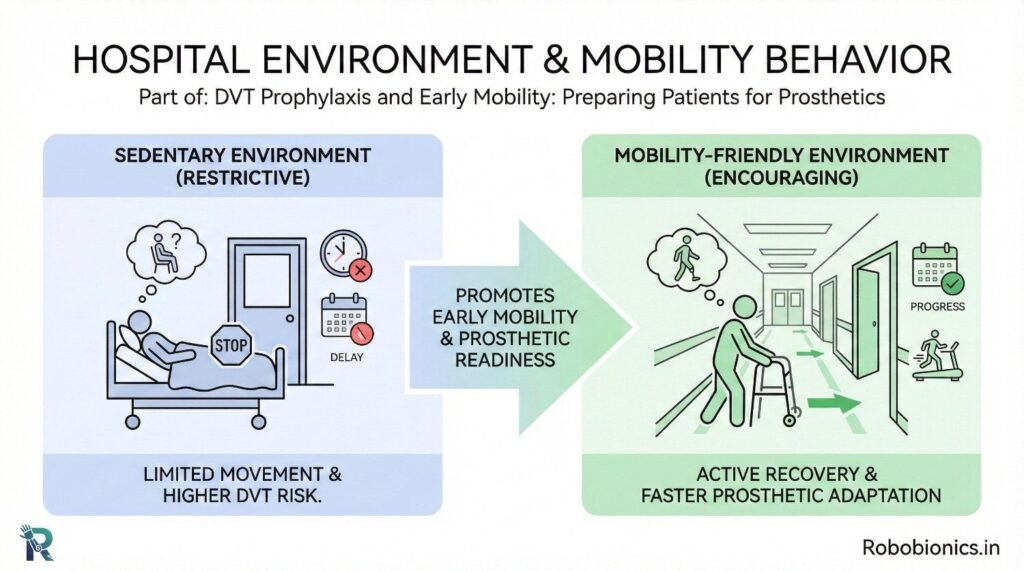
Crowded rooms, poor lighting, and lack of handrails discourage movement. A supportive environment encourages safe activity.
Design affects behavior.
Walkers, chairs, and support bars must be easily available. Delays in access delay movement.
Tools enable action.
When staff encourage movement, patients follow. When staff seem rushed or cautious, patients hesitate.
Tone influences trust.
Early mobility should be tracked as a care quality measure. Patients who move early have better outcomes.
Movement reflects care quality.
Tracking time to standing, walking, and rehab start helps predict prosthetic success. These metrics matter.
Data guides improvement.
Regular review of mobility outcomes helps teams refine protocols.
Learning improves systems.
Patients who move early learn prosthetic control faster. Their body adapts more easily to new movement patterns.
Prepared bodies learn better.
Early standing helps patients accept weight through the limb. This reduces fear during prosthetic trials.
Confidence improves alignment.
Stronger patients tolerate longer training sessions. This accelerates progress.
Endurance supports success.
Early movement helps patients see themselves as active individuals, not passive patients.
Identity shapes effort.
Mobility allows patients to leave the bed, interact with others, and feel normal.
Connection supports healing.
Movement shows progress. Progress builds hope.
Hope fuels recovery.
Advanced prosthetics require strength, balance, and endurance. Early mobility builds these foundations.
Preparation expands options.
Patients delayed by DVT or immobility may lose eligibility for advanced devices.
Early care protects choice.
Prepared patients can handle more functional prosthetics.
Readiness defines fit.
Mobility goals should carry from hospital to rehab without reset. Gaps slow progress.
Continuity builds momentum.
Rehab teams should know what the patient has achieved and what is safe.
Clarity prevents regression.
Habits built early should continue.
Consistency supports independence.
DVT prevention and early mobility are not separate from prosthetic care. They are the foundation on which prosthetic success is built. When blood flow is protected and movement begins early, patients retain strength, confidence, and readiness.
A prosthesis does not restore movement on its own. The body must be prepared to receive it. Early care decisions decide whether that preparation succeeds.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body