
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


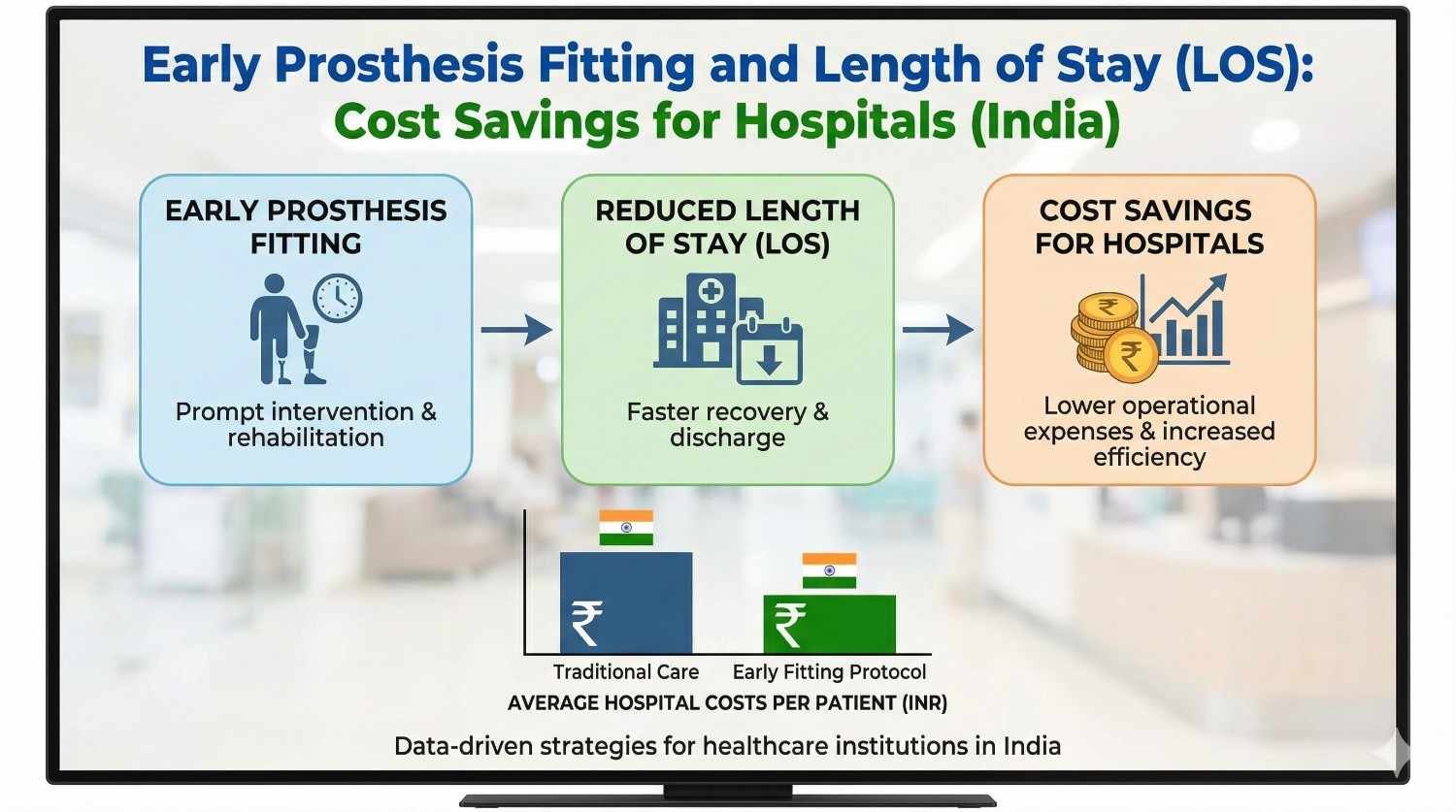
Length of stay is one of the quiet drivers of hospital cost in India. Every extra day in a bed affects staffing, capacity, cash flow, and patient experience. For amputee care, one decision has a surprisingly strong impact on length of stay: how early a prosthesis is planned and fitted.
This article is written for hospital leaders, surgeons, rehab heads, and care coordinators who want practical ways to reduce length of stay without cutting corners on care. We will explore how early prosthesis fitting changes recovery timelines, lowers inpatient burden, and creates real cost savings for Indian hospitals. The focus will stay simple, evidence-based, and rooted in what actually works on the ground.
In Indian hospitals, beds are always in demand.
Emergency admissions, trauma cases, and elective surgeries compete for the same limited space.
When one patient stays longer than expected, it affects the entire admission flow.
Length of stay is therefore not just a metric, but a daily operational pressure.
Each additional inpatient day adds costs for nursing, meals, housekeeping, and utilities.
These costs are often fixed and difficult to reduce in the short term.
When length of stay increases, margins shrink quietly.
Hospitals feel this pressure most in high-volume departments.
Long hospital stays increase patient frustration and anxiety.
Families face higher travel and accommodation costs.
The longer a patient stays, the higher the risk of dissatisfaction.
Reducing LOS improves both cost control and experience.

Amputation patients often remain admitted until wounds are stable and mobility begins.
Without a clear prosthetic plan, rehab progress slows.
Patients wait for confidence, balance, and basic function.
This waiting period extends length of stay significantly.
Many hospitals still follow a delayed prosthetic pathway.
The focus stays on healing first, function later.
While well-intended, this approach often creates idle inpatient days.
These days add cost without adding value.
Physiotherapy without a prosthesis has limits.
Patients can strengthen muscles but cannot practice real walking or balance.
This creates a rehab plateau.
LOS stretches while progress slows.
Early prosthesis fitting does not mean ignoring wound care or safety.
It means planning prosthetic intervention from the start.
Temporary or preparatory prostheses can be used safely.
The goal is to restore function as soon as possible.
Traditional care is sequential: surgery, healing, rehab, prosthesis.
Early fitting allows parallel planning.
Healing and functional training happen together.
This overlap shortens total recovery time.
When patients know that walking will begin early, motivation improves.
They engage better with therapy.
Fear and uncertainty reduce.
Psychological readiness supports faster discharge.
With early fitting, patients begin weight-bearing and balance training sooner.
Functional mobility improves earlier in the admission.
Once basic independence is achieved, discharge becomes possible.
Early prosthetic use keeps rehab moving forward.
Therapy sessions focus on real tasks instead of exercises alone.
Progress becomes visible and measurable.
Visible progress supports earlier discharge decisions.
Doctors and families feel more confident sending patients home when they can stand or walk.
Early prosthetic success reduces fear of falls.
Confidence accelerates discharge planning.
Confidence saves days.
Each avoided inpatient day saves variable and semi-fixed costs.
While exact numbers vary, savings accumulate quickly at scale.
In high-volume centers, even one day less per patient matters.
Early fitting delivers repeatable savings.
Shorter stays free beds sooner.
This allows hospitals to admit new patients faster.
Improved bed turnover increases revenue potential.
Capacity is used more efficiently.
Shorter LOS reduces nursing and therapy load per patient.
Staff can focus on acute needs instead of prolonged care.
This improves morale and efficiency.
Operational stability improves.
Multiple studies show that early mobility improves outcomes after amputation.
Hospitals observe faster functional milestones with early prosthetic planning.
LOS reduction is a consistent finding.
The pattern is clear across settings.
Indian hospitals adopting early fitting report smoother discharge flows.
Rehab teams see fewer stalled cases.
Administrators note better bed availability.
Experience supports evidence.
In systems with limited beds and high demand, benefits multiply.
Each saved day has higher opportunity cost.
Early fitting therefore has outsized value in India.
Context amplifies impact.
Some teams worry that early prosthetic use risks wound issues.
With proper protocols, these risks are manageable.
Temporary sockets and close monitoring reduce complications.
Fear often outweighs evidence.
Early fitting requires coordination between surgery, rehab, and prosthetics.
Without clear pathways, delays occur.
Hospitals need defined roles and timelines.
Coordination is key.
Some administrators worry about upfront prosthetic cost.
However, LOS savings often exceed these costs.
Budget thinking must shift from line items to total cost.
Early investment creates net savings.
Not every patient is suitable for early fitting.
Clear criteria help teams select appropriate cases.
Stable wounds and medical status are key.
Selection protects outcomes.
Early involvement allows timely assessment and planning.
Prosthetists can prepare temporary solutions in advance.
This reduces waiting time later.
Early engagement saves days.
Rehab teams should link milestones to discharge readiness.
Standing, transfers, and short-distance walking become targets.
Once targets are met, discharge follows.
Clear goals prevent drift.
Shorter hospital stays reduce direct expenses for families.
Travel, food, and lodging costs drop.
Economic stress reduces.
This improves satisfaction.
Patients recover better at home once basic mobility is achieved.
Home-based rehab becomes possible earlier.
This supports long-term recovery.
Early discharge benefits both sides.
When recovery feels fast and purposeful, trust grows.
Families perceive efficiency and competence.
This strengthens hospital reputation.
Reputation has long-term value.

Many hospitals agree with early prosthesis fitting in principle, but struggle to apply it consistently on the floor.
The gap usually lies not in clinical skill, but in workflow design and timing.
Early fitting works best when it is treated as a standard pathway, not a special case that depends on individual initiative.
Hospitals that formalize the process see more reliable reductions in length of stay.
One of the biggest delays in amputee care comes from late decisions.
When prosthetic planning starts only after wound healing, valuable inpatient days are already lost.
Early fitting requires that the decision to plan for a prosthesis is made within the first few days after surgery.
This early clarity allows all teams to work toward the same discharge timeline.
Traditional thinking separates healing and function into two phases.
In reality, healing and functional recovery can progress together when managed carefully.
Early prosthesis fitting supports circulation, posture, and confidence, which can actually aid recovery.
Hospitals that adopt this mindset see smoother patient journeys.
Surgeons play a key role in enabling early prosthetic pathways.
Clear communication about wound stability, weight-bearing limits, and expected healing timelines helps downstream teams plan effectively.
When surgeons flag suitable patients early, unnecessary waiting is reduced.
This clarity directly affects length of stay.
Rehab teams are often the first to notice when progress stalls.
Without a prosthesis, therapy sessions focus on strength but lack functional translation.
Early fitting gives therapists a tool to accelerate mobility training.
This makes rehab more purposeful and discharge-oriented.
In hospitals where prosthetists are involved only after discharge, delays are common.
Early fitting works best when prosthetists are treated as part of the inpatient care team.
Bedside assessments, early casting, and temporary solutions reduce waiting time later.
Integration improves speed without compromising safety.
Early fitting does not require a final, permanent prosthesis in most cases.
Temporary or preparatory prostheses are designed specifically for early rehab.
They allow basic standing, transfers, and short walks while the limb continues to heal.
This approach balances safety with speed.
Temporary prostheses are easier to adjust as limb volume changes.
They reduce the risk of fit-related skin issues during early recovery.
Most importantly, they unlock functional training that would otherwise be delayed.
From an LOS perspective, their value is significant.
Early fitting does not create extra work later when planned well.
Data collected during the temporary phase helps refine the final prosthesis.
Patients are already trained and confident by the time of definitive fitting.
This continuity supports both clinical and operational efficiency.

Concerns about wound breakdown are common and valid.
Early fitting protocols include strict wound assessment and gradual loading.
Close monitoring allows issues to be caught early.
In practice, complications are rare when protocols are followed.
Not every amputee is a candidate for early fitting.
Medical stability, wound condition, and cognitive readiness matter.
Clear inclusion and exclusion criteria protect patients and programs.
Selective use improves overall success rates.
Early prosthesis programs require attentive staff.
Nurses and therapists should be trained to spot redness, discomfort, or gait issues early.
Prompt adjustments prevent escalation.
Safety and speed can coexist when teams are prepared.
Below-knee amputees often benefit the most from early fitting.
Balance and gait training progress quickly with a temporary prosthesis.
Many patients achieve basic independence within days instead of weeks.
LOS reductions in this group are often substantial.
Above-knee amputees traditionally have longer stays due to balance challenges.
Early fitting helps patients learn transfers and controlled standing earlier.
While full walking may take longer, discharge readiness improves sooner.
Even partial gains reduce inpatient days.
Trauma patients are often younger and more motivated, making early fitting smoother.
Vascular patients require more careful monitoring but still benefit when selected properly.
Both groups show LOS improvement when early pathways are applied appropriately.
Contextual adaptation matters more than diagnosis alone.
Average length of stay can hide important details.
Hospitals should also track how many patients exceed expected LOS.
Early prosthesis fitting often reduces these outliers.
Reducing long-stay cases has a strong financial effect.
Tracking LOS alongside functional milestones gives better insight.
Hospitals can see how early standing or walking correlates with discharge timing.
This data helps refine pathways further.
Measurement drives improvement.
Clear data helps convince skeptical stakeholders.
When teams see consistent LOS reduction, buy-in increases.
Success becomes self-reinforcing.
Evidence builds momentum.
One of the most effective leadership conversations compares costs directly.
The cost of early prosthetic services is often lower than the cost of a few extra bed days.
When framed this way, the financial logic becomes clear.
LOS savings usually outweigh upfront investment.
Early fitting makes discharge timelines more predictable.
Predictability improves staffing, scheduling, and capacity planning.
Hospitals value stability as much as savings.
Early prosthesis programs deliver both.
Over a year, small LOS reductions compound.
More patients can be treated with the same infrastructure.
This improves access and revenue without expansion.
Throughput gains are a strategic advantage.
Programs fail when early fitting depends on individual enthusiasm.
It must be embedded into standard pathways.
Consistency matters more than occasional success.
System design beats heroics.
Late referrals to prosthetics undo early gains.
Assessment and planning should happen early, even if fitting is staged.
Delay is the enemy of LOS reduction.
Early engagement is critical.
Discharge planning should begin on admission.
Early prosthesis fitting supports this by giving clear functional goals.
Waiting until the end wastes valuable days.
Backward planning saves time.

Standing and walking early reduce fear dramatically.
Patients feel progress and hope.
This psychological shift improves cooperation with discharge plans.
Confidence accelerates recovery.
When families see early mobility, they gain confidence in home care.
This reduces resistance to discharge.
Education during the inpatient stay smooths transition.
Prepared families shorten LOS.
Early fitting should be framed as a step, not a miracle.
Clear expectations prevent disappointment.
Honest communication builds trust.
Trust supports smoother discharge.
Hospitals that succeed with early prosthesis fitting treat it as a default pathway for eligible patients.
This means documenting early fitting in clinical protocols rather than leaving it to individual preference.
When early fitting is written into standard care, teams act faster and with more confidence.
Consistency at the system level is what delivers reliable length of stay reduction.
Not every amputee should be fitted early, and clarity protects outcomes.
Hospitals should agree on basic eligibility markers such as wound stability, medical status, and cognitive readiness.
Clear criteria reduce hesitation and prevent inappropriate cases.
Safety and speed work together when boundaries are clear.
One of the strongest predictors of early discharge is how soon prosthetic planning begins.
Hospitals should set a clear trigger, such as prosthetist assessment within 48 to 72 hours after surgery.
Early assessment allows time for preparation without rushing fitting.
This early start saves days later.
Prosthetists should not function as external service providers.
Including them in rounds or case discussions aligns timelines and expectations.
This integration reduces miscommunication and waiting.
Shared planning improves discharge flow.
Communicate wound expectations and weight-bearing limits early and clearly.
Flag suitable patients for early fitting as soon as possible.
Avoid default delays unless clinically required.
Clear surgical guidance accelerates downstream care.
Shift therapy goals toward functional milestones linked to discharge readiness.
Use early prosthetic trials to break rehab plateaus.
Document progress clearly to support discharge decisions.
Functional focus reduces LOS.
Prepare temporary or preparatory prostheses quickly and safely.
Plan for limb volume changes and early adjustments.
Maintain close communication with rehab and nursing teams.
Responsiveness supports early success.
Monitor skin, comfort, and patient confidence during early use.
Report issues early to prevent setbacks.
Support patient education and confidence building.
Nursing vigilance protects both safety and speed.

Leadership should frame early prosthesis fitting as both a quality and cost initiative.
When clinical teams understand the financial value of reduced LOS, support increases.
Shared goals reduce resistance.
Alignment drives adoption.
Hospitals should track LOS for amputee patients before and after early fitting adoption.
Sharing this data builds trust and momentum.
Visible improvement encourages continued effort.
Measurement reinforces success.
Some upfront investment may be needed for prosthetic services or coordination.
Leadership should view this as a tool to unlock larger downstream savings.
Reinvestment supports sustainability.
Smart investment fuels efficiency.
Internal proposals should compare the cost of early prosthetic services with the cost of extra bed days.
This simple comparison resonates strongly with decision-makers.
Avoid overloading proposals with complex data.
Clarity persuades better than volume.
Hospitals unsure about full adoption can start with pilot groups.
Pilots allow teams to learn and adapt.
Early success builds broader support.
Small starts lead to big change.
Concerns about safety, cost, or workload should be discussed openly.
Sharing evidence and local results reduces fear.
Transparency builds trust.
Trust enables change.
Patients who walk earlier feel hopeful and motivated.
Early success improves overall recovery experience.
Satisfied patients speak positively about care.
Experience matters as much as outcomes.
Early prosthesis pathways encourage teamwork across departments.
Clear roles and timelines reduce friction.
Collaboration improves efficiency across other pathways too.
Culture change spreads benefits.
Hospitals known for efficient amputee care attract referrals.
Better throughput improves access without expansion.
Reputation grows quietly but steadily.
Efficiency becomes a competitive advantage.
Length of stay is one of the few cost levers hospitals can control without compromising care.
Early prosthesis fitting is a practical, patient-centered way to use this lever.
When planned thoughtfully, it shortens stays, improves outcomes, and strengthens hospital operations.
The value is both clinical and financial.
At RoboBionics, we work closely with Indian hospitals and see the difference early prosthetic planning makes every day.
Hospitals that integrate prosthetics early into the care pathway move patients forward faster and free resources for others who need them.
Early prosthesis fitting is not about doing more work sooner; it is about doing the right work at the right time.
When hospitals make this shift, length of stay falls, confidence rises, and care becomes more efficient for everyone involved.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body