
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Cancer-related amputations change life in a moment, but the care journey that follows lasts for years. For hospitals and oncology teams, the challenge is not only to remove disease, but to restore movement, dignity, and hope as early as possible. The timing of prosthetic care plays a much bigger role in this journey than many systems realize.
This article explores oncology amputation pathways with a clear focus on cost. We will examine how early prosthetic integration affects recovery speed, complications, rehabilitation effort, and long-term spend. The goal is to show, in simple and practical terms, why earlier prosthetic planning is not just a clinical choice, but a smart economic one for hospitals and care networks.
Oncology amputations are planned around cancer control, not sudden injury.
Surgery timing, margins, and reconstruction all depend on tumor behavior.
This planning window creates a rare opportunity to integrate prosthetic care early.
Unlike trauma cases, there is often time to prepare the patient and the system.
When this time is not used, costs rise later in less visible ways.
Many oncology patients receive chemotherapy or radiation before or after amputation.
These treatments affect healing, strength, and skin quality.
Delayed healing increases hospital stay and follow-up cost.
Early prosthetic planning can reduce these delays by aligning rehab with treatment cycles.
Cancer patients often enter amputation already weakened by treatment.
Fatigue, weight loss, and fear are common.
When mobility is delayed, this weakness deepens.
Early movement supports both physical recovery and emotional stability.
In many hospitals, prosthetic care begins months after surgery.
Teams wait for full healing, oncology clearance, and patient readiness.
During this waiting period, patients remain immobile.
This immobility quietly increases cost through complications and longer rehab.
Delayed mobility often leads to longer inpatient rehab.
Muscle loss and poor balance take time to reverse.
Each extra rehab day adds cost and uses capacity.
These costs are rarely linked back to prosthetic timing, but they should be.
Immobility increases the risk of joint stiffness, back pain, and falls.
Cancer patients are especially sensitive to these setbacks.
Treating secondary issues adds visits, imaging, and therapy.
Many of these costs are preventable with earlier integration.
Early integration does not mean rushing to fit a prosthesis.
It means involving prosthetic teams before surgery happens.
Pre-surgical planning supports better limb shaping and scar placement.
These details reduce future fitting issues and adjustment costs.
Early integration often uses temporary or preparatory prosthetics.
These allow safe standing and short walks during healing.
Even limited early movement reduces muscle loss and fear.
This shortens the overall rehab timeline.
When prosthetic milestones align with chemo or radiation schedules, care flows better.
Patients avoid long inactive gaps between treatments.
This coordination reduces dropouts and delays.
Smooth pathways lower total cost.
Every week of immobility leads to muscle weakening.
Rebuilding strength takes more therapy than maintaining it.
Therapy cost rises sharply when patients start from zero.
Early prosthetic use preserves baseline strength.
Patients who delay walking lose natural movement patterns.
They develop compensations that are hard to correct.
Correcting poor gait takes time and specialist input.
Early walking prevents many of these habits.
Cancer patients already face emotional strain.
Extended immobility can lead to depression and withdrawal.
Mental health support, longer rehab, and poor engagement all add cost.
Early movement protects motivation and confidence.
Patients who stand and walk earlier progress faster in therapy.
They need fewer total sessions to reach independence.
This reduces direct rehab cost and frees capacity.
Hospitals benefit from improved throughput.
Early mobility improves circulation and lung function.
This lowers the risk of clots, infections, and falls.
Each avoided readmission represents major savings.
These savings often exceed the cost of early prosthetic care.
When recovery timelines shorten, beds turn over faster.
Staff time is used more efficiently.
Early integration improves operational flow.
Flow improvements have strong financial impact.
Cancer treatment often causes weight changes.
Prosthetics must adapt to these shifts without full replacement.
Modular and adjustable designs reduce refit cost.
Flexibility protects budgets over time.
Radiation and chemotherapy affect skin health.
Sockets must reduce pressure and heat buildup.
Protective designs lower wound risk.
Wound prevention saves both money and time.
Early prosthetic stages focus on safety, not speed.
Stable designs reduce fall risk during recovery.
Avoiding early falls prevents setbacks.
Prevention here has very high return.
Oncology, surgery, rehab, and prosthetics often work separately.
This separation creates delays and duplication.
Early integration forces collaboration.
Collaboration reduces waste and improves outcomes.
When no one owns the full pathway, costs scatter.
Assigning pathway ownership improves accountability.
Clear leadership ensures early prosthetic steps happen on time.
Timeliness reduces downstream expense.
When teams share recovery milestones, decisions align.
Cost discussions become easier when goals are common.
Alignment reduces friction and delay.
Delay is expensive.
Patients who see a clear mobility plan feel hopeful.
Hope improves participation in rehab.
Engaged patients progress faster.
Faster progress reduces cost.
Uncertainty drives extra visits and calls.
Early prosthetic planning provides clarity.
Clear plans reduce unnecessary utilization.
Lower utilization supports better margins.
Patients remember systems that supported them early.
Trust improves follow-up and adherence.
Better adherence means fewer complications.
Fewer complications protect budgets.
Early standing is a strong predictor of recovery speed.
Hospitals should track this milestone.
Faster milestones often mean lower total cost.
Simple metrics reveal powerful trends.
Patients with early integration often need fewer sessions.
Tracking session counts shows clear differences.
Lower rehab intensity without worse outcomes proves value.
Data supports continued investment.
Long-term mobility and independence matter.
Early integration often leads to better long-term use.
Better long-term use reduces repeat interventions.
Long-term savings matter.
Some teams delay prosthetics fearing wound issues.
With proper planning, early care can be safe.
Education and protocols reduce fear.
Fear-based delay is costly.
Early prosthetic cost may sit in one department.
Savings appear in another.
Leadership must look at total cost, not silos.
Whole-pathway views enable smarter decisions.
Without protocols, early integration depends on individuals.
This creates inconsistency.
Standard pathways reduce variability.
Consistency reduces cost.
Early prosthetic planning should be standard, not special.
Standard care delivers predictable outcomes.
Predictable outcomes support stable budgets.
Stability benefits everyone.
Better care and lower cost are not opposites here.
They move in the same direction.
Early integration proves this alignment.
It is both humane and practical.
Cancer care does not end in the operating room.
Mobility is part of healing.
Hospitals that restore movement early restore lives faster.
That is the real value of early prosthetic integration.
Early prosthetic integration starts with a simple shift in thinking. Prosthetics should be discussed before surgery, not after discharge. When oncology teams involve prosthetists during pre-surgical planning, decisions improve across the pathway.
Surgeons can shape the limb with future prosthetic use in mind. Scar placement, bone length, and soft tissue handling all affect long-term fit. Small choices made in the operating room can reduce months of adjustment later.
This early coordination reduces refits, skin issues, and therapy delays. Each avoided problem represents both a clinical win and a cost saving.
Cancer patients often feel their care is uncertain. Treatments come in phases, with waiting periods in between. Early prosthetic planning introduces structure into this uncertainty.
A clear mobility timeline shows patients when they will stand, when they will walk, and how rehab will progress alongside cancer treatment. This clarity improves participation and reduces anxiety-driven care use.
From a cost view, structured timelines reduce missed appointments, repeated assessments, and stalled rehab stays.
Temporary prosthetics are not final solutions, but they are powerful tools. They allow safe standing and early weight bearing while healing continues.
Even limited use keeps muscles active and joints flexible. This reduces the intensity and duration of later rehabilitation.
Hospitals that use temporary solutions effectively often see smoother transitions to definitive prosthetics, with fewer setbacks and lower total spend.

The largest costs in oncology amputations rarely come from the prosthetic itself. They come from extended rehab, complications, readmissions, and prolonged dependence.
Early prosthetic integration shifts spending away from crisis care toward planned care. Planned care is easier to budget and control.
When hospitals map costs across the full journey, early investment often proves cheaper than delayed action.
Oncology care already works in phases. Surgery, recovery, adjuvant therapy, and surveillance each have defined periods.
Prosthetic care should align with these phases. Early integration distributes cost more evenly instead of concentrating it later during intensive rehab.
This alignment improves cash flow predictability and reduces sudden budget pressure.
Patients without clear mobility plans often seek extra consultations, second opinions, or emergency care due to fear or uncertainty.
Early prosthetic integration reduces this behavior by setting expectations and milestones. Fewer unplanned visits mean lower indirect cost and less system strain.
Cancer-related fatigue and inactivity quickly reduce muscle strength. When prosthetic use begins early, even at low intensity, this decline slows.
Preserved strength means rehab focuses on skill building rather than basic conditioning. Skill-based rehab is faster and less resource-intensive.
This difference has a direct impact on therapy cost and length of stay.
Many oncology amputees fear movement after surgery. Pain, weakness, and uncertainty combine to create hesitation.
Early supported standing and walking rebuild trust in the body. When fear reduces, progress accelerates.
Faster progress lowers therapy hours and improves discharge readiness.
Patients who achieve basic mobility earlier are easier to discharge safely. Home adaptations, caregiver training, and follow-up planning become simpler.
Smooth discharges reduce delayed bed days, which are costly and disruptive.
Patients who integrate prosthetic use early are more likely to continue using it long term. They develop habits, confidence, and skill early in recovery.
Long-term use supports independence and reduces reliance on wheelchairs, caregivers, and medical support.
Over years, this sustained use lowers cumulative healthcare cost.
Immobility increases the risk of heart disease, weight gain, and mental health issues. These conditions add long-term cost far beyond amputee care.
Early mobility protects overall health. Healthier patients use fewer services over time.
This broader impact is often overlooked in cost discussions.
Better early fit and training reduce the need for major revisions later. Patients adapt gradually instead of compensating poorly.
Avoided revisions save surgical, inpatient, and rehab costs.
Hospitals that perform oncology amputations benefit from dedicated pathways rather than case-by-case planning.
Clear protocols define when prosthetic teams are involved, how temporary devices are used, and how rehab progresses.
Standard pathways reduce variability, which is a major cost driver.
Waiting for wound closure or oncology clearance often delays prosthetic planning unnecessarily.
Clear referral triggers, such as post-surgical stabilization or initial healing milestones, keep care moving.
Timely referrals reduce idle time, which adds hidden cost.
When oncology, rehab, and prosthetic appointments are coordinated, patients move smoothly through care.
Poor coordination leads to missed windows, repeated assessments, and duplicated work.
Coordination improves efficiency and patient satisfaction.

Early integration does not mean ignoring wound safety. It means designing protocols that protect healing while allowing movement.
Partial weight bearing, protective sockets, and close monitoring reduce risk.
With the right safeguards, early care can be both safe and effective.
Some teams worry that prosthetic focus distracts from cancer treatment. In practice, early mobility often supports treatment tolerance.
Active patients cope better with chemotherapy and radiation. They recover faster between cycles.
Mobility and oncology goals can support each other.
Early integration fails when teams are unsure how to proceed. Training and shared protocols build confidence.
Confidence reduces unnecessary delay, and delay is costly.
Cancer often removes control from patients. Early prosthetic planning gives some of it back.
When patients feel involved in recovery, they engage more actively. Active engagement improves outcomes and reduces wasted effort.
Engagement is a cost-saving force.
Movement improves mood, sleep, and motivation. These benefits reduce demand for mental health services and crisis care.
Better mental health also improves rehab participation.
The financial impact of psychological stability is real, even if indirect.
Patients who feel supported early develop trust in the hospital. Trust improves follow-up adherence and reduces conflict.
Fewer conflicts and complaints reduce administrative cost and legal risk.
Early prosthetic care may increase upfront spending in one department. Savings appear later in others.
Hospitals must track total episode cost to see the true picture.
Whole-pathway measurement supports smarter leadership decisions.
Hospitals unsure about early integration can start with small pilot programs. Comparing outcomes builds internal evidence.
Data from real patients convinces teams better than theory.
Pilots reduce fear and accelerate adoption.
Early integration pathways should evolve with experience. Regular review improves both care quality and cost control.
Learning systems outperform static ones.
Early prosthetic integration aligns clinical excellence with financial sense. It reduces waste while improving lives.
Few interventions offer this level of alignment.
Hospitals that adopt it lead in both care and efficiency.
Healthcare is moving toward bundled payments and outcome-based reimbursement. Early integration fits these models well.
It reduces complications and variability, which are punished in value-based systems.
Early adopters gain an advantage.
Oncology amputations will always be complex. But complexity does not require delay.
Hospitals that restore movement early set a higher standard of care.
That standard benefits patients, teams, and systems alike.

Across oncology centers that plan prosthetics early, a clear pattern appears. Patients begin standing sooner, often within weeks of surgery, even if only for short periods.
These patients regain confidence faster. They engage better with physiotherapy and tolerate cancer treatment with less fatigue.
From a cost view, their rehab phase is shorter and more focused. They require fewer unplanned visits and fewer corrective interventions later.
In delayed pathways, patients often remain wheelchair-bound for months. Muscle loss, fear of movement, and poor balance become entrenched.
When prosthetic care finally begins, rehab must first undo decline before building skill. This adds time, staff effort, and frustration.
These patients show higher rates of falls, joint pain, and readmissions. The cumulative cost is significantly higher, even though initial spending was lower.
The biggest difference appears over time. Early integration creates momentum that carries forward. Delayed care creates drag that persists.
Each delay increases the effort needed to recover. Each setback adds cost that cannot be recovered later.
Cost differences compound quietly, but powerfully.
Early integration pathways show fewer total therapy sessions. Sessions focus on function rather than basic conditioning.
Delayed pathways require longer therapy blocks. More staff hours are needed to reach the same outcome.
Rehab cost often exceeds prosthetic cost. This makes timing a major financial lever.
Patients who mobilize early have fewer secondary issues such as back pain, falls, and wound breakdown.
Delayed patients return more often for preventable problems. Each return triggers imaging, consults, and sometimes admission.
Avoiding even a small number of readmissions creates major savings.
Early planning supports better initial fit. Better fit reduces the need for major revisions.
Delayed integration often leads to poor early habits and compensations. These habits increase wear and alignment issues later.
Revision surgeries and major refits are costly and disruptive.
Shorter rehab stays free up beds for other patients. This improves hospital throughput.
In high-demand oncology centers, bed availability has direct revenue impact.
Early integration improves flow without increasing capacity.
When recovery timelines are consistent, staffing and scheduling become easier.
Predictability reduces overtime, burnout, and inefficiency.
Stable systems cost less to run.
Early integration forces teams to work together regularly. Over time, this collaboration becomes smoother.
Reduced friction saves time and reduces error.
Collaboration is a hidden efficiency driver.
Patients from distant locations or with limited support are more likely to drop out when care is delayed.
Early integration anchors them into a clear pathway before motivation fades.
This reduces loss to follow-up and wasted initial investment.
Cancer treatment is exhausting. Asking patients to restart mobility months later increases dropout risk.
Early steps keep patients engaged while motivation is high.
Engagement protects outcomes and cost.
When prosthetic care is introduced early and explained clearly, it feels like part of treatment, not an extra burden.
This framing improves acceptance and adherence.
Acceptance improves value.

Early integration does not happen by accident. It requires leadership support.
Without leadership, departments default to caution and delay.
Leadership sets expectations that timing matters.
If one department bears early cost while another gains later savings, resistance grows.
Leaders must align incentives to reflect total pathway value.
Aligned incentives enable smart decisions.
Early integration requires trained teams and clear protocols.
Investment in people and process delivers more value than equipment alone.
Capability reduces long-term spend.
Standardization reduces variability, but clinical judgment remains essential.
Well-designed pathways guide timing while allowing flexibility.
Balance supports both safety and efficiency.
Tracking outcomes and cost over time allows refinement.
Learning systems improve with each case.
Improvement protects margins and patients.
Once proven, early integration models can be scaled to other sites.
Scaling spreads cost savings and quality gains.
System-wide impact follows.
For many cancer patients, amputation threatens identity as much as function.
Early movement helps restore a sense of self.
This emotional recovery supports physical recovery.
Hope changes behavior. Patients who believe they will walk again try harder.
Early prosthetic exposure builds realistic hope.
Hope accelerates healing.
Helping patients stand and move early preserves dignity.
Dignity reduces resistance, fear, and disengagement.
Dignity has economic value.
It replaces delay, inefficiency, and reactive care.
It reorganizes cost around prevention and momentum.
Replacement is cheaper than repair.
This pathway does not cut care. It improves it.
Better care reduces waste, duplication, and harm.
Cost control follows quality.
Oncology amputation care will continue to evolve.
Early prosthetic integration should be part of that future.
Hospitals that adopt it now lead in value, compassion, and sustainability.
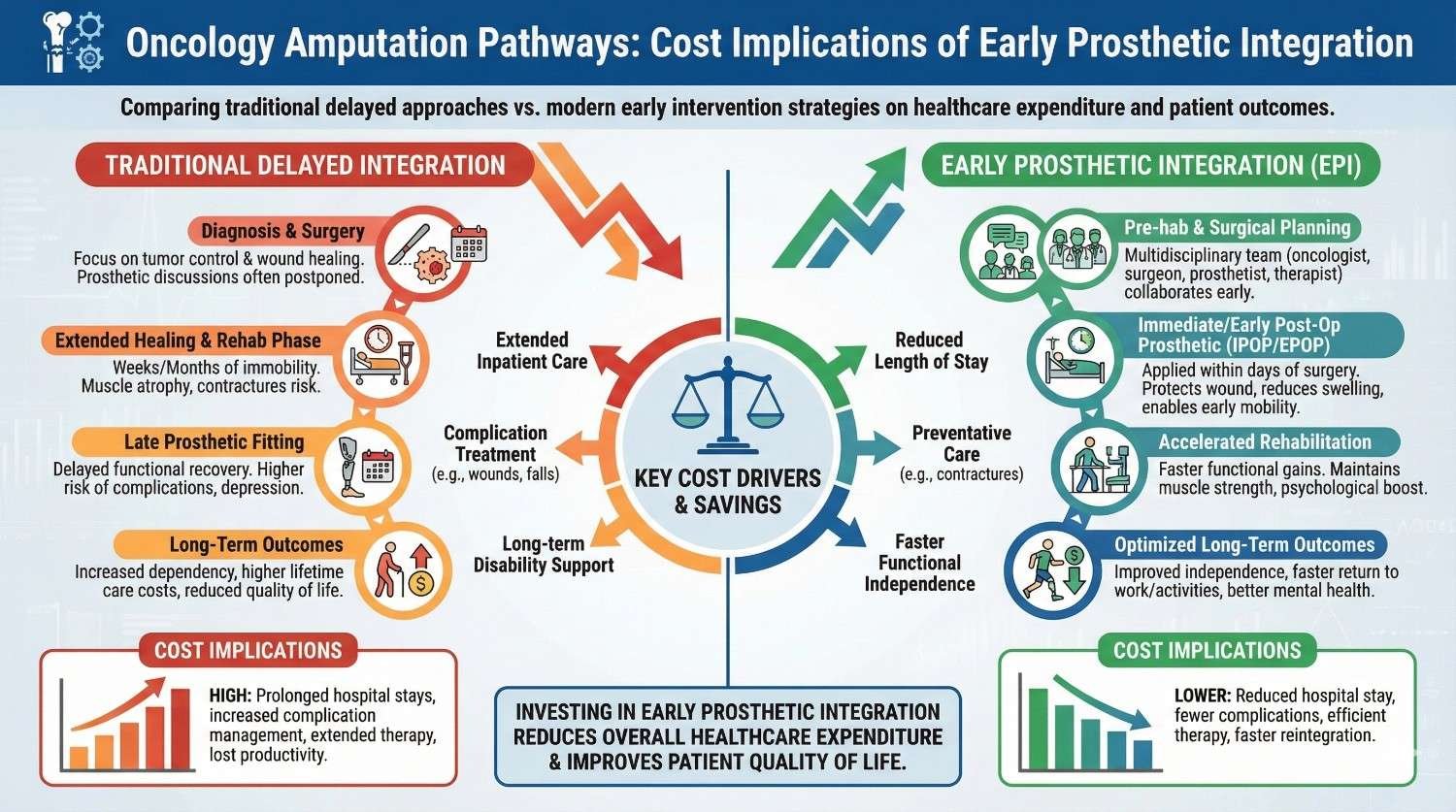
Oncology-related amputations are planned, high-cost, and emotionally intense episodes of care. Unlike trauma cases, hospitals often have time to plan these pathways. Yet in many systems, prosthetic care still begins late, after healing, after oncology clearance, and after prolonged immobility has already caused decline.
This delay quietly drives cost. Longer rehabilitation, higher complication rates, repeated therapy cycles, delayed discharge, and long-term dependency all add up. Early prosthetic integration is one of the few interventions that improves outcomes while lowering total episode cost.
Early prosthetic integration does not mean rushing to a final prosthesis. It means planning mobility before surgery, introducing temporary or preparatory prosthetics during recovery, and aligning rehabilitation with oncology treatment timelines.
When this happens, patients stand sooner, walk sooner, and recover faster. The financial impact shows up not as a single saving, but as a reduction across multiple cost drivers that hospitals already struggle to control.
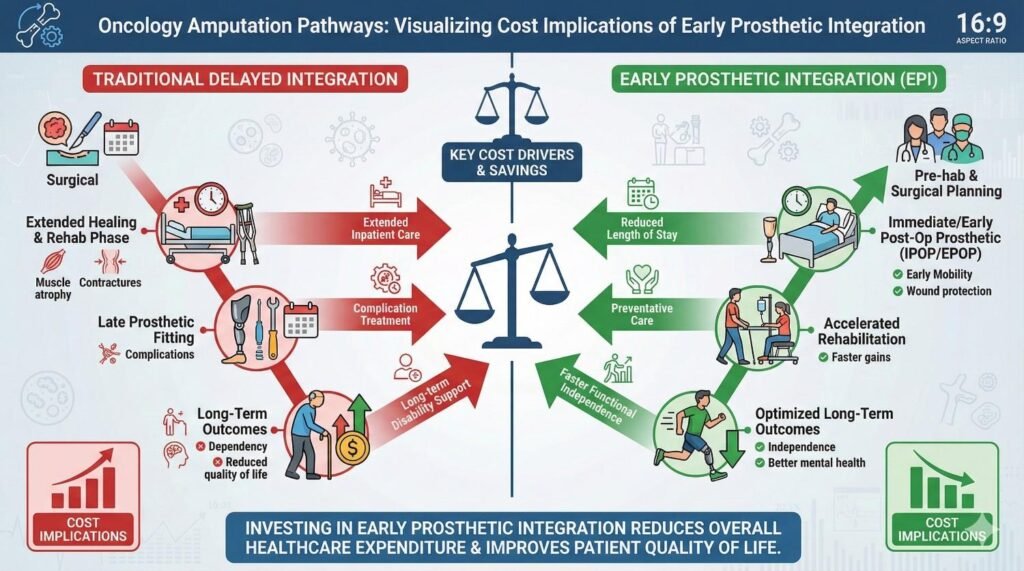
In oncology amputations, the prosthetic device itself is rarely the largest expense. The biggest costs usually come from:
Prolonged inpatient and outpatient rehabilitation
Delayed discharge and blocked beds
Readmissions due to falls, weakness, or secondary issues
Revision fittings caused by poor early limb shaping
Long-term mobility decline leading to higher care dependence
Early integration directly reduces each of these areas.
Patients who begin supported standing and early walking preserve muscle strength and joint movement. They relearn balance before fear and compensation patterns set in. They stay mentally engaged during cancer treatment instead of withdrawing.
This leads to faster functional gains, fewer therapy sessions, and safer discharge. These clinical improvements are the foundation of the economic benefit.
Hospitals that adopt early prosthetic integration typically see:
Shorter rehabilitation timelines
Lower total therapy hours per patient
Fewer unplanned visits and readmissions
More predictable recovery pathways
Better bed utilization and throughput
While prosthetic-related spending may appear earlier in the pathway, total episode cost is lower when measured end to end.
Delayed prosthetic care creates a compounding effect. Every week of immobility increases the effort and cost required later. Rehab shifts from skill training to basic reconditioning. Fear of movement grows. Complications become more likely.
Once decline sets in, it is expensive to reverse. Early integration prevents this decline instead of paying to fix it.
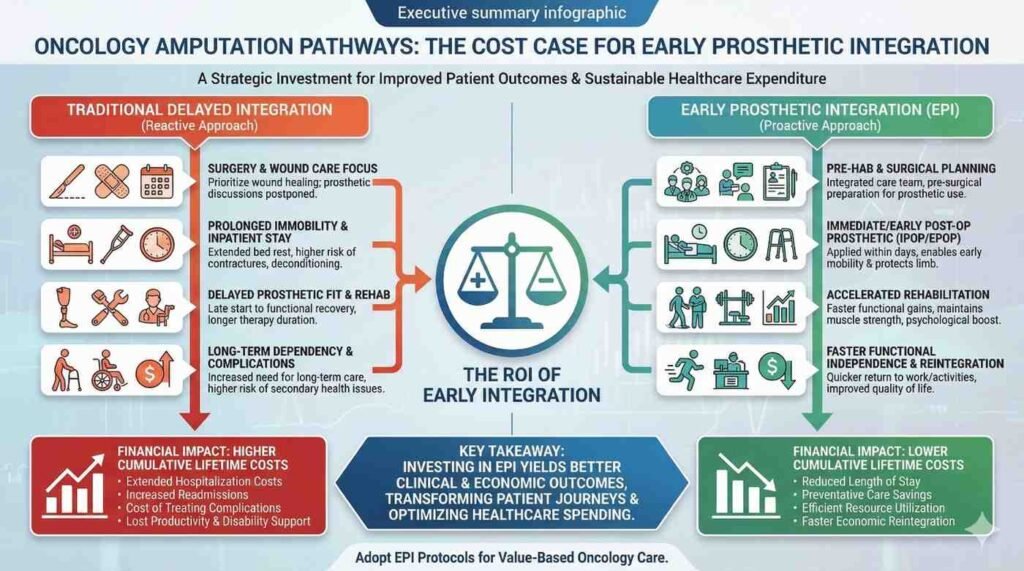
Early prosthetic integration does not fail because it is unsafe or ineffective. It fails when leadership allows timing decisions to default to habit, fear, or departmental silos.
Successful hospitals treat early integration as a pathway decision, not a prosthetics decision. They measure total episode cost, not line-item spend. They align incentives across oncology, surgery, rehab, and prosthetics.
Healthcare is moving toward bundled payments, value-based reimbursement, and outcome accountability. Early prosthetic integration reduces variability, complications, and length of care, all of which are penalized in modern payment models.
Hospitals that adopt this approach early are better prepared for future reimbursement structures.
Early movement restores dignity, confidence, and hope at a time when cancer patients feel most vulnerable. These human outcomes drive better engagement, better adherence, and better long-term use of prosthetic care.
Better engagement always lowers cost.
Early prosthetic integration in oncology amputations is not an added cost. It is a cost reallocation from late, reactive care to early, preventive care.
Hospitals that move prosthetic planning upstream reduce total spend, improve patient experience, and strengthen system efficiency. This is one of the rare cases where better care and better economics move in the same direction.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body