
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation



Prosthetic care for children is not a smaller version of adult care. It is a long-term medical decision that must grow with the child’s body, mind, and daily life. For doctors, the challenge is not only deciding if a child can use a prosthesis, but also when to introduce it, how to support learning, and how to adapt as the child develops. Timing mistakes in pediatric prosthetics can affect movement patterns, confidence, and social development for years.
This article explains pediatric prosthetic indications with a clear focus on growth, cognition, and timing, written for MDs working in real clinical settings. It brings together medical judgment, developmental understanding, and practical experience to help doctors make safe, ethical, and child-centered decisions. The aim is to support healthy development, functional independence, and emotional well-being from early childhood through adolescence.
Children are still growing in body, brain, and emotions, which means prosthetic decisions affect future development, not just current function.
A choice that works today may need revision within months as height, weight, and movement patterns change.
Doctors must think in years, not weeks, when planning pediatric prosthetic care.
Motor skills, balance, and coordination develop in stages during childhood.
A prosthesis should support these stages rather than interrupt them.
Understanding normal child development helps avoid delays caused by poor timing.
Children born with limb differences often adapt naturally from infancy.
Those who lose a limb later must relearn movement and body image.
These two groups need different timing and counseling approaches.
Infants and toddlers grow quickly, with frequent changes in limb length and body proportion.
Prostheses at this stage are often simple and used mainly for balance and body awareness.
The goal is exposure, not performance.
Between ages five and twelve, growth happens in bursts.
Socket fit and alignment can change suddenly during these periods.
Regular monitoring is essential to prevent discomfort or gait issues.
Teenagers approach adult height but still experience changes in muscle strength and coordination.
Prosthetic needs often shift toward function, appearance, and independence.
Timing upgrades carefully helps maintain confidence during this sensitive phase.
Young children must grasp that movement of the body affects the prosthesis.
This understanding develops gradually through play and repetition.
Cognitive readiness matters as much as physical readiness.
Children have limited attention, especially at younger ages.
Training must be short, playful, and consistent.
A prosthesis should never feel like punishment or pressure.
Children learn best by watching and copying others.
Peer interaction and play-based therapy improve prosthetic use.
Structured drills alone rarely work in pediatric care.
In upper-limb differences, early fitting helps the brain include the prosthesis in body mapping.
Even if function is limited, early exposure supports coordination.
This approach is common in infants and toddlers.
Some children function well without a prosthesis in early years.
Fitting may be delayed until a clear functional or social need appears.
Delaying does not mean denying care.
Pressure from parents or society can lead to early fitting before readiness.
Rushed decisions increase rejection and frustration.
Timing should follow the child, not expectations.
Children have delicate skin that can break down easily under pressure.
The residual limb must tolerate gentle loading without redness or pain.
Skin health should be checked frequently.
Good joint movement supports natural gait and posture.
Imbalances can worsen with growth if not addressed early.
Physiotherapy plays a key role before and after fitting.
Children tire quickly during learning.
Fatigue affects posture, safety, and mood.
Prosthetic use should fit naturally into daily routines.
Children become aware of differences as they grow.
A prosthesis can support confidence or increase self-consciousness, depending on timing.
Doctors should watch for emotional signals during consultations.
School-age children often face questions or staring from peers.
Prosthetic decisions should consider social comfort, not only function.
Counseling and peer exposure can help.
Teenagers may resist prosthetics due to appearance or social pressure.
Respecting their voice is essential for long-term acceptance.
Forced use often leads to rejection.
Parents often drive early prosthetic decisions.
Doctors must guide them toward child-centered choices.
Education reduces fear and unrealistic expectations.
Children depend on adults for skin checks and maintenance.
Caregiver ability affects prosthetic safety.
Support systems must be assessed early.
Teachers and caregivers influence daily use.
Simple awareness can prevent stigma or misuse.
Collaboration improves outcomes.
In early years, exploration matters more than precise function.
Touching, holding, and moving are valid goals.
Doctors should redefine success at each age.
Children benefit from trying tasks independently, even imperfectly.
A prosthesis should support independence, not restrict it.
Small gains matter.
Older children should have a say in design and use.
Choice increases ownership and pride.
This approach improves long-term engagement.
We have now covered the foundations of pediatric prosthetic indications, focusing on growth, cognition, timing, and family involvement.
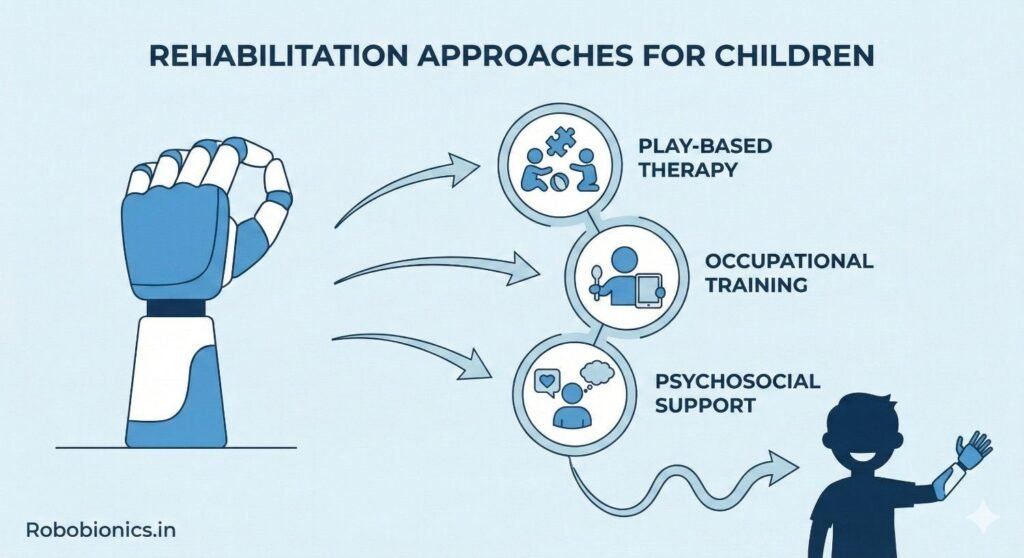
Rehabilitation for children works best when it feels like play and routine rather than treatment.
Short sessions woven into daily activities keep children engaged without pressure.
This approach supports learning while protecting emotional well-being.
Physiotherapy helps with balance, posture, and safe movement as the child grows.
Occupational therapy supports hand use, play skills, and school tasks.
Close coordination between doctors and therapists improves timing decisions.
Growth spurts can temporarily disrupt coordination and comfort.
Therapy plans should slow down or shift focus during these periods.
Flexibility prevents frustration and injury.
School is often the first place where children compare themselves to peers.
A prosthesis can support participation, but only if the child feels ready.
Doctors should discuss school timing during candidacy decisions.
Children may face questions or staring from classmates.
Preparing the child with simple responses builds confidence.
Teacher awareness helps create a supportive environment.
Sports and play are important for development.
Prosthetic use during these activities should be gradual and supervised.
Safety matters more than performance.
Early fitting has benefits, but it is not always the best choice.
Some children thrive without a prosthesis in early years.
Individual assessment prevents unnecessary rejection.
Children, especially adolescents, may resist if they feel unheard.
Listening to their concerns builds trust.
Forced use often leads to long-term abandonment.
Children outgrow sockets and components quickly.
Missed follow-ups lead to discomfort and poor use.
Regular review is a core part of pediatric eligibility.
What works at age three may not work at age eight.
Doctors should expect multiple transitions over time.
Reassessment protects both function and confidence.
Poor gait or posture can become habits if not corrected early.
Regular observation helps prevent long-term strain.
Early correction is easier than later repair.
As children grow, goals shift toward independence.
Prosthetic planning should evolve with these goals.
Long-term care is a journey, not a single decision.
Adolescents often care deeply about how they look.
Prosthetic design and appearance influence acceptance.
Respecting these concerns improves use.
Teenagers should gradually take responsibility for care and decisions.
This prepares them for adult prosthetic management.
Guided independence builds confidence.
Transition planning should begin before full adulthood.
Clear handover between pediatric and adult care teams matters.
Continuity reduces dropouts.
Doctors must balance parental wishes with the child’s needs.
Decisions should support long-term development, not short-term pressure.
Ethics guide timing as much as medicine.
Children should not be labeled as poor candidates too early.
Development is dynamic and unpredictable.
Keeping options open respects potential.
As cognition improves, children should be included in decisions.
This builds trust and responsibility.
Shared choices improve adherence.
There is no single right age for prosthetic fitting.
Readiness depends on growth, learning, and environment.
Doctors must reassess timing regularly.
Success may mean participation, confidence, or comfort rather than skill.
Child-centered outcomes matter most.
These outcomes guide better decisions.
Pediatric prosthetic care extends over many years.
Doctors guide families through change and growth.
Consistency builds trust and success.
At Robobionics, we work closely with pediatric doctors, therapists, and families across India.
We understand that children need prosthetic solutions that grow with them, adapt to learning, and respect emotional development.
By combining careful timing, child-friendly design, and ongoing support, we aim to help doctors restore movement, confidence, and joy at every stage of childhood.
We are now approaching the next major word milestone.
In infancy, prosthetic indication is less about function and more about helping the child develop early body awareness, symmetry, and balance, so that the brain learns to include the prosthetic side as part of normal movement from the very beginning.
Devices at this stage are usually simple, light, and easy to tolerate, and they are introduced gradually through supervised play rather than structured training.
Doctors should focus on comfort, safety, and exposure, while clearly explaining to parents that active use may be limited and that this is both normal and acceptable.
Between ages three and five, children begin to explore their environment with more purpose, and prosthetic indications often relate to play, self-care, and basic participation rather than skill or strength.
Cognitive growth during this phase allows children to start understanding simple cause-and-effect relationships, which supports more intentional prosthetic use.
Timing decisions should consider attention span, curiosity, and the child’s natural interest in using both sides of the body during play.
As children enter school, prosthetic goals often shift toward participation in classroom activities, social play, and early independence, making functional indications more visible and meaningful.
Growth spurts during this phase can quickly change socket fit and comfort, so doctors must plan for frequent review and adjustment.
Prosthetic use should support learning and confidence, not distract the child from school or create unnecessary pressure.
A child’s ability to plan, remember, and problem-solve directly affects how well they learn prosthetic movement, especially for upper-limb devices or more complex lower-limb control.
Children with delayed cognitive development may still benefit from prosthetics, but expectations must be adjusted and training simplified.
Eligibility should reflect learning capacity rather than age alone.
Young children can become frustrated quickly when tasks feel difficult or unfamiliar, which may lead to avoidance of the prosthesis if sessions are too demanding.
Doctors should encourage short, positive interactions with the prosthesis that end in success rather than exhaustion.
Emotional regulation improves with age, and prosthetic plans should evolve alongside it.
Children learn best through repeated exposure in familiar settings, which makes daily routines more effective than occasional long therapy sessions.
Prosthetic use during dressing, eating, or play helps the brain build automatic patterns.
Consistency over time is a stronger predictor of success than intensity.
As children grow older, they become more aware of physical differences and may compare themselves to peers, which can influence their willingness to use a prosthesis in public.
Doctors should watch for subtle signs of discomfort or withdrawal during visits.
Social readiness is a valid part of prosthetic timing decisions.
A supportive school environment often improves prosthetic acceptance more than any technical adjustment.
Simple education for teachers and classmates can reduce stigma and curiosity.
Doctors can guide families on when and how to introduce these conversations.
Children should be encouraged to join activities at their own pace, without forcing prosthetic use in every situation.
Allowing choice helps children feel in control rather than judged.
This approach supports long-term acceptance.
Rapid growth means that sockets may become uncomfortable or unsafe within months, which can frustrate families if expectations are not set early.
Doctors should clearly explain that frequent changes are part of pediatric care, not a failure of the device.
Planning ahead reduces emotional and financial stress.
Some children temporarily avoid prosthetic use during growth spurts due to discomfort or coordination changes.
This phase should be managed with patience rather than enforcement.
Reintroduction often succeeds once growth stabilizes.
Poor alignment or discomfort during growth can lead to compensatory movement patterns that persist into adulthood.
Regular observation and early correction protect long-term musculoskeletal health.
This is one of the most important medical responsibilities in pediatric prosthetic care.
Upper-limb prosthetics in children often focus on bilateral activity, body symmetry, and social comfort rather than pure strength or precision.
Early exposure helps the brain integrate the device, even if active use is limited at first.
Doctors should reassess function regularly as fine motor skills develop.
Lower-limb prosthetic indications are closely tied to balance, walking safety, and participation in play.
Children generally adapt quickly, but growth can disrupt gait patterns unexpectedly.
Ongoing gait observation is essential.
Children with multiple limb differences or additional conditions need highly individualized plans.
Prosthetic timing may differ for each limb.
Coordination between specialties improves outcomes.
As children approach adolescence, prosthetic goals often shift toward independence, appearance, and social integration.
Doctors should gradually involve the child more directly in decision-making.
This prepares them for adult prosthetic care.
The move from pediatric to adult care is a vulnerable period where many patients disengage.
Early planning and clear communication reduce this risk.
Continuity supports long-term success.
Success in pediatric prosthetics should be measured over years, not months.
Participation, confidence, and health matter more than technical perfection.
This long view protects both child and family well-being.
Pediatric prosthetic indications require patience, flexibility, and respect for growth, learning, and emotion, because children are constantly changing in ways that no single plan can fully predict.
Doctors play a central role not only in deciding when to fit a prosthesis, but also in guiding families through adjustment, expectation, and long-term adaptation.
When timing, cognition, and growth are respected together, prosthetics can become tools that support development, confidence, and independence rather than obstacles to childhood.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body