Pre-Prosthetic Physiotherapy: Medical Prescriptions That Improve Outcomes
Pre-prosthetic physiotherapy is one of the most powerful yet underused tools in amputation care. Long



When a person stops using a prosthetic, it is often seen as failure. Many assume the device did not work or the patient did not try hard enough. In reality, this moment deserves deeper attention, not blame. A failed prosthetic experience is not the end of the journey. It is a signal that something needs to be understood better.
At Robobionics, we have met many patients who come to us after putting their first prosthetic aside. They arrive with disappointment, doubt, and sometimes guilt. Our experience shows that most of these cases do not fail because of lack of effort. They fail because the first selection did not match the patient’s real needs, body, or life.
This article explains why reassessment after failed prosthetic use is medically important. It explores how doctors should approach second-line selection with care, clarity, and respect. We will explain what to re-evaluate, how to rebuild trust, and how better choices can be made the second time.
Failed prosthetic use does not always mean the patient rejected the idea of using a prosthesis. In many cases, the patient wanted it badly but could not continue because daily use became painful, tiring, or emotionally stressful.
This distinction is important. When failure is misunderstood, the reassessment starts on the wrong foot and repeats old mistakes.
Some patients stop using a prosthetic for a short time. Others stop completely. These two situations are very different.
Temporary breaks often signal overload or poor training. Complete disuse usually points to deeper issues that were never addressed in the first selection.
Prosthetic abandonment is more common than most people admit. Many patients quietly stop using their device without informing the clinic.
This silence hides learning opportunities. Doctors must normalize discussion around failure to improve outcomes.
When a prosthetic fails, patients often lose trust in technology and clinicians. They may feel misled or unheard.
This emotional injury must be healed before any second-line decision can succeed.
Many patients blame themselves. They believe they did not try hard enough or lacked discipline.
This belief damages confidence and reduces openness during reassessment.
Patients approach reassessment with fear. They worry the second prosthetic will fail again.
Doctors must acknowledge this fear openly instead of rushing into solutions.
Advanced features often attract attention during first selection. However, complexity without readiness leads to frustration.
A prosthetic that looks impressive may not suit daily life.
Some assessments focus only on physical fit and ignore lifestyle, work, and emotional readiness.
This gap becomes visible only after the patient returns home.
When patients expect fast results, normal struggles feel like failure.
Clear expectation setting is often missing in first-line selection.
Second-line selection is not about choosing a different device quickly. It is about understanding what went wrong.
Without this understanding, reassessment becomes guesswork.
Patients must feel safe to speak openly about discomfort, fear, and dissatisfaction.
Reassessment should feel like support, not evaluation.
Every failed prosthetic holds valuable lessons.
Doctors must treat reassessment as a learning process.
The reassessment should begin with listening, not measurements.
Patient stories reveal patterns that reports cannot show.
Questions should invite honesty, not defensiveness.
How did the prosthetic feel during daily tasks is more helpful than why did you stop using it.
Patients may express anger or sadness.
Allowing this expression builds trust and clears the path forward.
The body changes over time. Skin condition, volume, and sensitivity may differ from the first fitting.
Second-line selection must start with a fresh physical assessment.
Pain points reveal design or fit issues.
Ignoring these signals risks repeating failure.
Muscle strength and endurance may be lower than expected.
The second prosthetic must respect current capacity, not ideal targets.
Doctors should review how the prosthetic performed in daily tasks.
Small frustrations often add up to abandonment.
A prosthetic that works in the clinic may fail at work or outdoors.
Environmental mismatch is a common reason for failure.
Early fatigue discourages regular use.
Understanding when and why fatigue occurred guides better selection.
Patients need time and reassurance before trying again.
Rushing this stage increases resistance.
Small achievable goals help rebuild belief.
Confidence must come before complexity.
Second-line success may look different from first expectations.
Doctors must help patients redefine what success means.
Motivation after failure is different from first-time motivation.
It may be quieter, cautious, and fragile.
Some patients return due to family pressure.
Doctors must ensure the desire is truly the patient’s own.
Gentle encouragement works better than strong persuasion.
Pressure recreates fear.
Second-line prosthetics often benefit from simpler design.
Ease of use builds confidence.
Comfort drives daily use.
Features matter only if they support comfort.
The goal is regular use, not occasional success.
Habits form through ease and predictability.
Clinicians must reflect on what influenced the first choice.
Honest review prevents repeated errors.
Second-line discussions should include clear timelines and limits.
This clarity protects trust.
Lessons from failure should be recorded.
This documentation guides future care.
Second-line prosthetics should be introduced gradually.
This reduces overload.
Goals should progress slowly.
Each success supports the next step.
Regular reviews catch issues early.
Early correction prevents abandonment.
Second-line selection should not begin with comparing brands or models. It should begin with a clear break from the thinking that guided the first choice.
Doctors must resist the urge to fix the old device’s problems with small tweaks. A fresh perspective leads to better outcomes.
The right second-line device fits naturally into the patient’s day. It supports how they live, work, travel, and rest.
If a prosthetic demands constant adjustment or attention, it slowly becomes a burden instead of support.
Many first failures are linked to weight or control complexity. What looks manageable in short trials becomes exhausting over full days.
Second-line devices should feel lighter in both body and mind.
Initial training programs are usually optimistic. They assume fast learning and steady progress.
After failure, training must become more realistic, flexible, and forgiving.
Second-line training benefits from slower progression. Patients need time to reconnect with their body and rebuild trust.
Deeper understanding replaces rushed performance.
Clinic-only training hides real challenges. Second-line users benefit from training that mirrors home and work tasks.
This realism prevents surprises later.
Trust cannot be rebuilt without acknowledging what went wrong.
Doctors should openly recognize the patient’s previous struggle without defensiveness.
Patients should not feel alone in failure. Shared responsibility builds partnership.
This shared approach encourages honesty and engagement.
Consistency in follow-ups, communication, and guidance rebuilds safety.
Predictability helps patients relax and commit again.
Painful skin problems quickly turn motivation into avoidance.
Second-line selection must prioritize skin tolerance above all else.
Socket issues are a leading cause of failure. Second-line care must reassess fit from the ground up.
Small changes in shape or material can create big comfort gains.
Patients should learn to recognize early discomfort.
Early reporting prevents serious injury and discouragement.
Second-line success is often quieter. It may not look dramatic.
Doctors must guide patients toward realistic, meaningful improvements.
Progress may show as longer wear time, less pain, or more confidence.
These signs matter more than complex movements.
Stable daily use is a strong success indicator.
Speed comes later, if at all.
After failure, many patients avoid wearing the prosthetic even when it fits better.
This fear must be addressed gently, not ignored.
Short, predictable routines help rebuild trust.
Gradual exposure reduces anxiety.
Easy access to support encourages continued use.
Silence often hides growing problems.
Families may become overprotective or skeptical after seeing failure.
Doctors must include them in reassessment discussions.
Unrealistic family pressure can push patients too fast.
Clear guidance protects the patient’s pace.
Families should support practice, not police it.
Balanced involvement strengthens confidence.
Fear after failure is normal. Patients should hear this clearly.
Normalization reduces shame and resistance.
A failed prosthetic can damage self-image.
Second-line care should support identity rebuilding alongside function.
Sometimes emotional readiness lags behind physical readiness.
Pausing is better than forcing progress.
Early comfort does not guarantee long-term success.
Regular long-term check-ins reveal true outcomes.
How often and how long the prosthetic is worn matters more than test scores.
Usage patterns reflect real acceptance.
Adjustments should feel normal, not corrective.
This mindset encourages honesty.
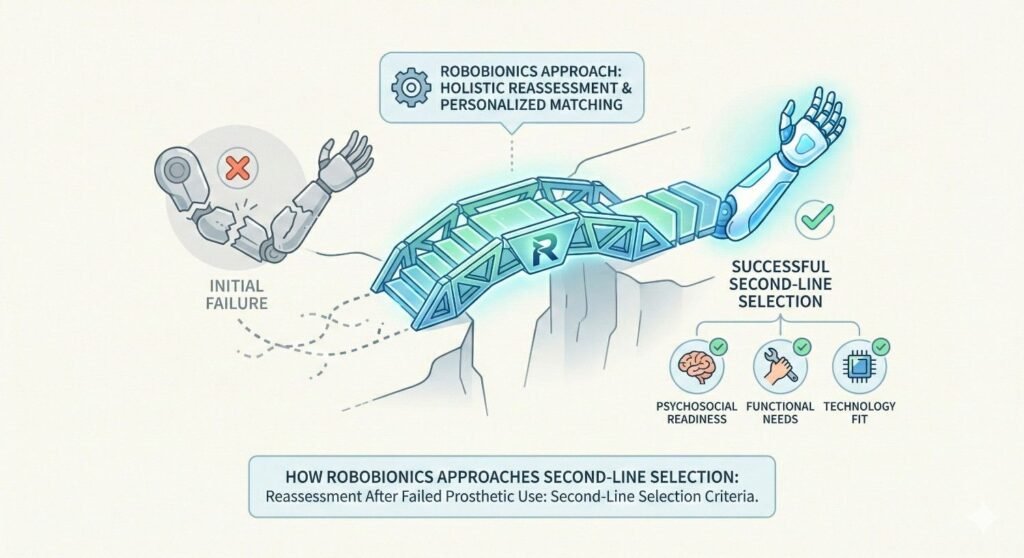
At Robobionics, we treat every failure as a learning opportunity.
We document insights to improve future care.
Our second-line solutions consider heat, travel, work conditions, and space limits.
Design must match reality, not ideals.
We stay connected with patients beyond fitting.
Ongoing support prevents silent abandonment.
A failed prosthetic experience should never be treated as a mistake to hide. It deserves respect and thoughtful response.
Doctors have an ethical duty to approach reassessment without judgment, urgency, or defensiveness.
Repeating the same approach after failure increases physical and emotional harm.
Ethical care demands that second-line decisions reduce risk, not simply offer another option.
Consent after failure must be deeper than the first time. Patients now carry fear and doubt.
Doctors must explain choices clearly and acknowledge past outcomes honestly.
Every failed prosthetic provides valuable feedback about selection, training, or support gaps.
Healthcare systems must treat this feedback seriously.
Lessons from second-line care should improve first-line decisions for future patients.
This loop reduces repeated failures over time.
Care models should expect some failures and plan for recovery.
This approach reduces stigma and improves trust.
Second-line success is not about erasing the past.
It is about moving forward with better understanding.
Comfort, safety, and confidence often matter more than advanced function.
These outcomes restore dignity.
Second-line journeys are often slower.
This pace supports deeper, lasting acceptance.
Failure can damage self-belief deeply.
Second-line care must rebuild belief step by step.
Goals after failure may change.
Doctors should support this shift without disappointment.
Not every patient will choose to continue.
Respecting this choice is part of dignified care.
Patients should feel confident asking for changes or support.
Self-advocacy prevents silent suffering.
Bodies and lives change.
Second-line plans must allow flexibility.
Patients should know they can pause without judgment.
This safety encourages honest use.
After failure, patients need steadiness more than excitement.
Calm guidance rebuilds trust.
False hope damages credibility.
Honest hope supports resilience.
Progress should match the patient’s comfort.
Doctors must adjust their pace accordingly.
Second-line care forces clinicians to listen more deeply.
This improves care quality overall.
Designers learn what truly matters in daily life.
This feedback leads to better prosthetics.
Acknowledging failure strengthens ethical standards.
It shifts focus from performance to people.
A failed prosthetic is not the end of the journey.
It is a turning point toward better understanding.
Good care adapts to reality.
Second-line selection reflects this maturity.
True success lies in dignity, comfort, and choice.
Second-line prosthetic care must always protect these values.
The time between stopping the first prosthetic and starting reassessment plays a major role in outcomes. Too short a gap may not allow emotional recovery. Too long a gap may allow fear and avoidance to grow.
Doctors should actively assess how time has affected both the body and the mind before planning second-line care.
Muscle strength, joint movement, and limb volume often change when a prosthetic is not used. These changes are not failures. They are natural responses to reduced activity.
Second-line selection must treat the body as it is now, not as it was during the first fitting.
Some patients need time to accept what happened. Others need reassurance quickly. There is no fixed rule.
Doctors must ask how the patient felt during the gap, not just how long it was.
After a failure, some clinicians swing too far toward extreme caution. They may limit function too much out of fear.
This can frustrate patients and reduce motivation. Balance is still required.
Fear can guide second-line decisions on both sides. Patients fear pain. Doctors fear repeat failure.
Acknowledging fear openly prevents it from quietly shaping poor choices.
Second-line selection should reduce risk without removing purpose.
The goal is safe progress, not permanent restriction.
Patients often forget details about why they stopped using a prosthetic. This is not dishonesty. It is human memory.
Structured reflection helps uncover patterns that memory alone misses.
Simple logs showing wear time, discomfort, and activity provide valuable insight.
These records guide second-line choices more accurately than opinions alone.
Small discomforts, skipped days, or mood changes often predict abandonment.
Doctors should take these signals seriously during reassessment.
Failure is often treated as embarrassment. This discourages honest reporting.
Healthcare systems must treat prosthetic failure as expected data, not personal fault.
Reassessment requires different skills than first fitting. Listening, patience, and humility matter more.
These skills should be taught, not assumed.
Patients should know what happens if the first prosthetic fails.
Clear pathways reduce fear and dropout.
Many families invest heavily in the first prosthetic. Failure creates financial stress and guilt.
Second-line care must respect this burden.
Second-line selection should prioritize durability, service access, and repair ease.
Sustainability matters more than novelty at this stage.
Hidden costs damage trust. Patients deserve clear financial discussions during reassessment.
Transparency reduces regret.
After failure, patients may ask for more advanced devices, believing technology will fix everything.
Without emotional readiness and comfort, even advanced devices fail.
Reassurance, consistency, and patience outperform features and specs.
Second-line success is more human than technical.
Second-line devices should reduce mental effort, not increase it.
Ease lowers emotional resistance.
A failed prosthetic experience changes a person. It changes how they see their body, their future, and the healthcare system meant to support them. It introduces doubt where there was once hope, and caution where there was once excitement. This is why reassessment after failed prosthetic use cannot be treated as a routine clinical step. It is a deeply human moment that demands respect, patience, and humility.
Second-line prosthetic selection is not about fixing a mistake quickly. It is about listening carefully to what the failure revealed. It asks doctors to pause, reflect, and accept that the first plan did not fit the person’s real life. This acceptance is not weakness. It is the foundation of better care.
For patients, failure often feels personal. Many believe they did something wrong. They question their effort, their strength, or their discipline. These beliefs quietly damage confidence and openness. If reassessment begins without addressing this emotional weight, even the best medical decision will struggle to succeed. Healing must begin with restoring dignity, not offering another device.
For doctors and clinicians, second-line care tests professional maturity. It requires moving away from defensiveness and toward curiosity. It demands honest reflection on selection criteria, training methods, and expectation setting. This is uncomfortable work, but it is essential. Medicine improves not by avoiding failure, but by learning from it openly.
True reassessment looks at the whole person again, without assumptions carried over from the first attempt. The body may have changed. The mind certainly has. Motivation may now be quieter, more cautious, but often more genuine. Readiness may be lower in some areas and stronger in others. Second-line care must meet the patient exactly where they are, not where they were expected to be.
Success after failure rarely looks dramatic. It often shows up in small, steady signs. Longer wear time without pain. Fewer excuses to avoid use. Greater comfort asking for help or adjustments. These signs matter deeply. They indicate trust returning, both in the device and in the care process.
At Robobionics, we believe second-line prosthetic care is not a backup plan. It is a refined, more honest phase of care. It allows patients and clinicians to strip away assumptions and focus on what truly matters: comfort, safety, confidence, and daily usefulness. Our experience across Indian homes, work environments, and climates has shown us that dignity grows when care becomes simpler, clearer, and more patient.
Second-line selection also reshapes the future of prosthetic care as a whole. Every reassessment teaches us how to select better the first time. It sharpens our understanding of real-world use. It reminds us that technology must serve humans, not impress them. This learning loop strengthens the entire system.
Most importantly, second-line care restores choice. It tells patients that they are not trapped by one outcome. That stopping once does not disqualify them from trying again. That pausing, changing direction, or redefining success is allowed. This freedom is powerful. It reduces fear and invites honest engagement.
A prosthetic is not just a medical device. It is something a person invites into their life, their routine, and their identity. When that invitation is withdrawn due to failure, it must be re-extended gently, with care and consent. Second-line selection, when done right, does exactly that.
In the end, reassessment after failed prosthetic use is not about proving that prosthetics work. It is about proving that healthcare listens. That it adapts. And that it places human dignity above timelines, targets, and pride. When care reaches this level, success follows naturally, not loudly, but lastingly.