
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much earlier, inside the ICU. Decisions made in the first few hours and days after injury often decide whether a patient reaches a prosthesis smoothly or faces months of delay.
Doctors working in trauma care carry a quiet but powerful influence over long-term outcomes. From limb handling and wound decisions to early communication and timing, every step shapes what comes next. When ICU care and prosthetic planning move in the same direction, recovery becomes faster, cleaner, and far more predictable.
This article is written for doctors who want to close the gap between life-saving trauma care and functional recovery. It focuses on clear, practical pathways that connect ICU management to prosthetic readiness. No complex words. No theory-heavy talk. Only what works in real hospitals, with real trauma patients.
Unlike planned amputations, trauma amputations happen without warning. The body and mind are pushed into crisis at the same time. Doctors must act fast to save life, often with little time to plan for function.
Because of this urgency, long-term recovery is rarely discussed in the early hours. Yet these early decisions quietly shape whether the patient reaches a prosthesis smoothly or struggles for months.
Most trauma amputees do not have a single injury. They may have head injury, chest trauma, fractures, or internal bleeding. The amputated limb becomes one part of a much larger problem.
In such cases, prosthetic planning feels distant. But ignoring it fully creates avoidable delays later. A balanced approach is needed, where survival comes first, but future function is not forgotten.
Trauma amputations involve crushed tissue, contamination, and irregular wounds. These factors increase infection risk and slow healing.
In the ICU, the focus is clear: stabilize the patient. Airway, breathing, circulation, and infection control take priority.
However, even during this phase, small choices matter. How the limb is positioned, how the wound is protected, and how swelling is managed all influence future outcomes.
Poor positioning in the ICU can lead to contractures and stiffness. These issues are difficult to reverse later and directly affect prosthetic use.
Simple steps, like neutral positioning and gentle support, protect future movement without interfering with critical care.
ICU care involves many specialists. When no one speaks about long-term limb function, it gets missed.
A short note or verbal update that flags “future prosthetic use” can change how the limb is handled throughout ICU stay.
In trauma, surgeons often revise amputations in stages. The initial level may change once the patient stabilizes.
Each revision should consider future prosthetic fitting. Preserving length when safe improves control and comfort later.
Good soft tissue coverage is essential for prosthetic sockets. Thin, fragile skin leads to pain and repeated breakdown.
Early planning for durable coverage saves time and suffering months later.
Trauma wounds are often contaminated. Aggressive cleaning and staged closure are common.
The goal is not speed, but stability. A clean, stable limb heals better and becomes prosthetic-ready sooner.
During the first three days, doctors focus on stabilization, infection control, and wound assessment.
This is also the best time to protect limb potential. Swelling control, gentle positioning, and clear documentation matter here.
Pressure points, tight dressings, and poor support can harm healing tissue.
Simple checks during rounds can prevent issues that later delay prosthetic fitting.
Early notes should include expected revision plans and long-term goals when possible.
This helps downstream teams understand the intent behind early decisions.
The move from ICU to ward feels like progress. However, this is where many plans fall apart.
If prosthetic goals are not carried forward, limb care becomes inconsistent.
The handover should include limb status, positioning needs, and movement precautions.
Mentioning “future prosthesis planned” keeps the goal alive across teams.
Once conscious and stable, patients begin to process what happened.
Early, sensitive conversations help prepare them mentally for the road ahead.
Waiting too long to start rehab is a common mistake. Even simple movements matter.
Early rehab protects joints, maintains muscle signals, and supports prosthetic control later.
Rehab does not mean pushing beyond safety. It means working within limits to protect function.
Doctors who guide rehab boundaries help therapists work confidently.
Joint stiffness and muscle loss start quickly. Early attention prevents long-term loss.
These early gains reduce prosthetic training time later.
Sudden limb loss is shocking. Fear, confusion, and grief are common.
Ignoring mental health slows physical recovery and prosthetic acceptance.
Short, honest conversations build trust. Patients do not need full answers immediately.
They need reassurance that recovery has a path.
Doctors should avoid timelines too early. Instead, focus on progress and steps.
This keeps hope realistic and strong.
Prosthetic planning does not mean fitting. It means preparation.
Even in the first week, doctors can flag patients who are likely candidates.
A simple early referral or discussion helps plan future care.
This avoids long waits once the limb is ready.
When doctors, therapists, and prosthetists share the same goal, care becomes smoother.
Alignment prevents mixed messages and delays.
In trauma amputees, infection is not just a medical complication, it is the single most common reason prosthetic fitting gets delayed by months. Even a small, persistent infection keeps the limb unstable and unsafe for socket fitting.
Doctors who treat infection aggressively and early do not just save tissue, they save time. A clean limb heals faster, tolerates pressure better, and progresses smoothly toward prosthetic readiness.
Most trauma amputations involve road injuries, industrial accidents, or crush injuries where dirt, grease, and foreign material are driven deep into tissue. Surface cleaning is never enough in these cases.
Early and repeated wound washouts, even when they feel excessive, often prevent deep infection later. Taking the time in the first few days reduces repeated admissions and revision surgeries down the line.
The pressure to close wounds early is understandable, especially when beds are limited. However, closing a wound that is not ready often leads to breakdown and infection.
Delayed or staged closure, when chosen wisely, supports better healing and faster prosthetic timelines overall, even if it feels slower in the short term.
In many trauma cases, the first surgery is about survival, not perfection. Tissue that looks viable initially may not survive later.
Planned revisions are not failures. They are part of smart trauma care. Doctors who explain this clearly to families reduce frustration and confusion later.
Preserving limb length is one of the strongest predictors of good prosthetic control. However, length should never be preserved at the cost of poor tissue quality.
Well-timed revisions that remove unhealthy tissue early often lead to a stronger, more usable limb that supports prosthetic fitting sooner.
Every surgery resets healing time. When revisions are not planned carefully, rehab progress gets interrupted repeatedly.
Doctors who align surgical plans with rehab goals help patients move forward without unnecessary stops.
Once patients leave the ICU, attention often shifts to discharge planning. This phase quietly shapes long-term outcomes.
Ward care is where habits form. How the limb is handled daily, how movement is encouraged, and how pain is managed all matter greatly.
Small skin issues often begin in the ward. Daily inspection helps catch problems early.
Consistency across shifts is critical. Mixed instructions lead to confusion and harm healing tissue.
Poor pain control leads to fear of movement. Over-sedation leads to inactivity.
Balanced pain management allows safe movement, which supports muscle signals needed for myoelectric prosthetics later.
Long ICU stays, splinting, and fear of movement create the perfect conditions for joint stiffness.
Once contractures form, they are difficult to reverse and often delay or limit prosthetic use permanently.
Positioning should not be left to chance. Neutral joint alignment must be maintained consistently.
Doctors who reinforce positioning during rounds send a clear message that function matters.
Movement does not mean stress. Even small, guided movements protect joints and muscles.
Clear medical boundaries help therapists work confidently without fear of causing harm.
Waiting for full comfort delays progress. Early rehab is about prevention, not performance.
Doctors who encourage early, gentle rehab reduce long-term stiffness and weakness significantly.
Vague instructions slow progress. Clear goals like “maintain joint range” or “protect muscle signals” guide therapy effectively.
This clarity helps therapists tailor sessions to future prosthetic needs.
Rehab should not happen in isolation. Short updates during rounds keep everyone aligned.
When rehab stalls, doctors can intervene early and adjust the plan.
Rushing to prosthetics with fragile skin often leads to pain and breakdown.
Doctors who prioritize skin strength over speed see better long-term outcomes.
Trauma limbs are often highly sensitive. Ignoring this leads to poor socket tolerance later.
Early desensitization strategies save weeks during prosthetic training.
Limb volume changes are expected. Tracking trends helps predict readiness.
Doctors who note volume patterns help prosthetic teams plan accurately.
Patients may seem stable one day and withdrawn the next. This is normal after trauma.
Doctors who recognize this avoid labeling patients as “uncooperative” and instead provide support.
What doctors say in early weeks stays with patients. Casual comments can create fear or false hope.
Thoughtful communication builds trust and resilience.
Patients recover better when they feel involved, not pushed.
Doctors who invite participation rather than demand it see better engagement.
Some doctors avoid mentioning prosthetics early, fearing emotional overload. In reality, uncertainty causes more distress.
Simple, future-focused conversations help patients see beyond the injury.
Prosthetics should be explained as a journey, not a single event.
This framing reduces frustration when fitting does not happen immediately.
Families often influence patient decisions strongly.
Early education prevents unrealistic expectations and pressure later.
Early referral does not lock the patient into a device or timeline.
It simply opens a channel for planning and guidance.
Prosthetic centers often have waiting periods. Early referral allows parallel planning.
When the limb is ready, the system is ready too.
Early collaboration builds respect and smoother handovers.
This trust improves outcomes for future patients as well.
When goals are not carried forward, care becomes fragmented.
Doctors who restate goals during transitions protect progress.
Minor redness, stiffness, or fear often signal bigger problems.
Early attention prevents late-stage delays.
Discharge is a transition, not an end.
Clear post-discharge plans protect prosthetic timelines.
In busy trauma settings, memory fails. Pathways provide reliability.
A clear pathway ensures key steps are never missed.
No two hospitals are the same. Pathways should fit available resources.
Simple, realistic pathways work better than perfect ones.
A pathway only works when everyone understands it.
Regular reinforcement keeps standards high.
For trauma amputees, discharge often feels like success. The patient is stable, the wound looks acceptable, and beds are needed for others. Yet this is one of the most dangerous points for prosthetic delay.
When discharge happens without a clear continuation plan, patients fall into gaps. Follow-ups get missed, wounds worsen quietly, and rehab slows down. What was gained in hospital can be lost within weeks.
Doctors must view discharge as a handover, not a finish line. Care is simply moving from one setting to another.
Clear instructions, fixed appointments, and named contacts make this transition safer. Patients and families should know exactly what happens next, not just that something will happen later.
Many patients believe discharge means they are close to getting a prosthesis. When this does not happen quickly, frustration builds.
Doctors should explain clearly that discharge means the body is healing well enough to continue recovery outside the hospital, not that prosthetic fitting is immediate. Honest words at this stage prevent anger and loss of trust later.
Once patients leave the hospital, outpatient follow-up becomes the main driver of recovery. This is where wounds mature, swelling settles, and readiness develops.
If follow-up is irregular or poorly guided, even a well-managed hospital course can end in long delays.
Open-ended advice like “come back in a few weeks” rarely works. Patients forget, delay, or wait until a problem appears.
Fixing the first two or three follow-up dates before discharge creates structure. It also signals that follow-up is part of treatment, not an optional extra.
Outpatient visits work best when they are coordinated. Seeing the surgeon, therapist, and prosthetic team in isolation often leads to mixed messages.
Doctors who help align these visits reduce confusion and speed up decision-making.
A wound that looks closed is not always ready for prosthetic load. Skin strength, scar quality, and tissue mobility matter greatly.
Doctors should assess not just appearance, but how the tissue behaves with light pressure and movement.
Trauma scars can become tight, painful, or uneven. If ignored, they make socket fitting difficult and uncomfortable.
Early scar care guidance during follow-ups saves weeks of delay later. This is a small effort with a large payoff.
Some wounds break down after initial healing, especially when swelling changes or activity increases.
Regular review during this phase catches problems early, before they force a complete pause in prosthetic planning.
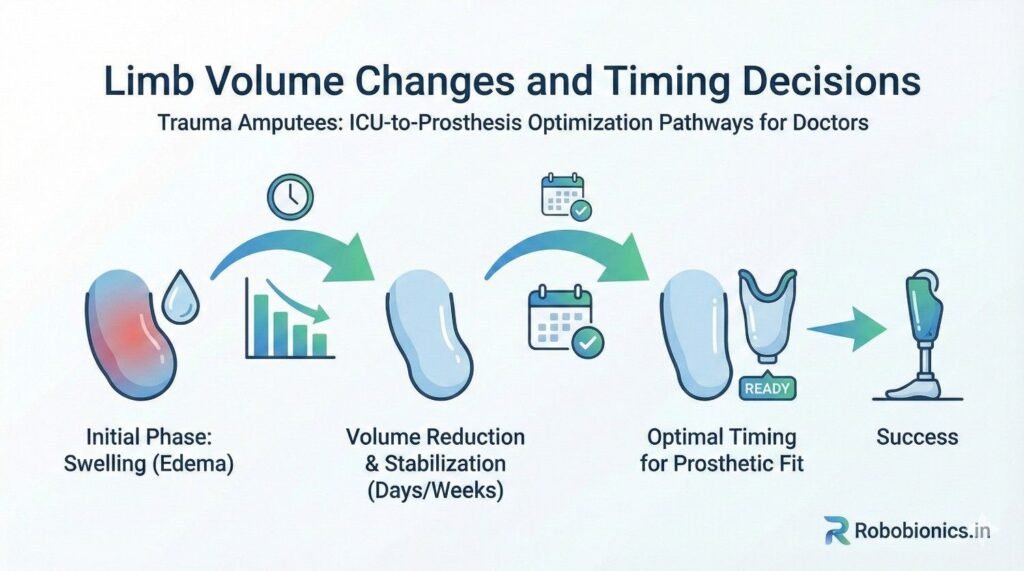
Trauma causes deep tissue damage. As healing progresses, swelling reduces in waves, not a straight line.
Doctors should expect fluctuation and plan around trends rather than single measurements.
Patients often get confused when told they are “almost ready” and then asked to wait longer.
Explaining that the limb is still changing helps them understand why waiting now prevents problems later.
Prosthetic fitting works best when volume is reasonably stable. Early communication about volume trends helps prosthetists choose the right time to act.
Doctors who share these insights reduce failed fittings and repeated visits.
For myoelectric prostheses, muscle signals are key. Trauma, pain, and immobility weaken these signals quickly.
Doctors should encourage early, safe muscle activation to preserve control potential.
Fear of pain or reinjury often leads patients to stop using the limb entirely.
Clear reassurance about safe movement helps maintain muscle function needed later.
Not all exercises support prosthetic control equally. Simple, targeted movements protect useful muscle patterns.
Doctors who communicate prosthetic goals help therapists design better programs.
There is no single test that says a patient is ready. Readiness is a mix of wound stability, skin tolerance, volume trends, movement, and mindset.
Doctors who look at the whole picture make better timing decisions.
Rushing leads to pain, breakdown, and rejection. Over-waiting leads to frustration and loss of motivation.
Balanced judgment, supported by regular reviews, protects outcomes best.
Simple tolerance checks, like light pressure or short wear trials, provide valuable information.
These small tests often guide timing better than visual inspection alone.
Once prosthetic fitting begins, some doctors step back completely. This can leave patients unsupported when issues arise.
Early prosthetic use often uncovers pain points that need medical input.
Skin irritation, discomfort, and fatigue are common in early use.
Doctors who support adjustment rather than stopping help patients adapt faster.
Patients may feel discouraged when prosthetic use feels harder than expected.
Reinforcement from doctors carries strong weight and helps patients stay committed.
Even after prosthetic fitting, the body continues to change. Weight shifts, muscle strength improves, and scars mature.
Long-term follow-up helps adjust care as the patient evolves.
Late skin issues, joint pain, or overuse injuries can appear if early patterns are poor.
Doctors who remain involved catch these issues before they limit function.
Success is not just physical ability. It includes comfort, confidence, and participation in daily life.
Doctors who ask about these aspects guide better long-term outcomes.
Even the best doctors struggle in broken systems. Pathways reduce dependence on individual memory and effort.
A clear pathway ensures that every trauma amputee receives consistent, future-focused care.
Pathways do not need to be perfect at launch. Simple steps that are followed consistently work best.
Regular review helps refine timing and communication.
ICU staff, ward nurses, therapists, and junior doctors all influence outcomes.
Shared understanding across teams keeps care aligned from day one.
Later often becomes too late. Early thinking does not mean early fitting, it means better planning.
Most patients prefer clarity over silence. Gentle, honest information reduces fear.
Waiting often causes stiffness and weakness that slow everything else.
Saving a life is the first victory. Helping that life regain function is the next.
Doctors shape this journey more than they often realize.
Positioning, timing, words, and follow-ups all add up.
Attention to these details shortens the road to prosthetic use.
Trauma amputees do best when life-saving care and future function move together.
Clear pathways turn chaos into progress.
In trauma care, survival is the first and most visible goal. However, for amputees, survival without function often leads to long-term dependence and loss of quality of life.
Doctors who look beyond discharge statistics and focus on functional recovery help patients return to work, family roles, and social life. These outcomes matter deeply to patients, even if they are harder to measure.
Every trauma patient heals at a different pace. Measuring success by fixed timelines often creates pressure and poor decisions.
Instead, outcomes should be tracked using functional milestones such as wound tolerance, joint movement, ability to sit or stand comfortably, and readiness to begin prosthetic training. These markers guide better clinical judgment.
When delays happen, they should be reviewed without blame. Was the delay due to infection, missed follow-up, poor coordination, or late referral?
Doctors and hospitals that track these patterns can improve pathways for future patients and reduce repeat delays.
At this stage, doctors should confirm that limb positioning is correct, swelling is managed, and long-term goals are documented.
Even a brief note stating “future prosthetic use anticipated” helps guide all downstream care.
In the ward, doctors should review whether movement is being encouraged safely and consistently across shifts.
This checkpoint helps prevent stiffness, muscle loss, and fear-driven inactivity.
Before discharge, doctors should confirm that follow-up appointments are fixed, rehab plans are clear, and the patient understands the next steps.
This checkpoint protects against the most common cause of long-term delay: loss of continuity.
During outpatient visits, doctors should assess readiness trends and confirm alignment with rehab and prosthetic teams.
This checkpoint ensures that when the limb is ready, the system is ready too.
Indian hospitals often manage a very high volume of trauma cases with limited staff and time.
In such settings, simple, repeatable pathways are more effective than complex protocols that are hard to follow consistently.
Many trauma amputees face sudden financial stress. Travel costs, lost income, and long treatment periods affect follow-up adherence.
Doctors who acknowledge these pressures can help plan realistic follow-up schedules and reduce dropouts.
In many regions, prosthetic services are not located near trauma hospitals. This physical gap creates delays.
Early referral and coordination help bridge this gap and reduce waiting once the patient is ready.
Family plays a major role in decision-making. Misunderstandings about prosthetics can slow acceptance.
Doctors who involve families early help create support instead of resistance.
Dropout is rarely due to lack of interest. More often, it is due to confusion, cost, fear, or unrealistic expectations.
Clear communication and structured follow-up reduce these losses significantly.
Too much information overwhelms patients. Simple explanations repeated over time work better.
Doctors should focus on what the patient needs to do next, not the entire journey at once.
When patients feel that the doctor is still invested in their recovery, they are more likely to return.
Small gestures, like checking progress or reinforcing goals, build this connection.
Doctors and prosthetists see different parts of the same journey. When they work in isolation, gaps form.
Collaboration reduces repeated assessments, mixed messages, and unnecessary delays.
Basic details such as injury mechanism, tissue quality, healing challenges, and patient motivation are extremely helpful.
Sharing these early improves prosthetic planning accuracy.
Regular collaboration builds mutual trust. Over time, teams learn each other’s strengths and constraints.
This trust leads to smoother care for every future patient.
Repeated exposure to severe injuries and long recoveries affects doctors deeply.
Acknowledging this reality helps prevent emotional exhaustion.
Clear pathways reduce the need to remember every detail for every patient.
Systems protect not only patients, but clinicians as well.
No single doctor should carry the entire burden of long-term recovery planning.
Team-based care spreads responsibility and improves consistency.
Clear digital records help maintain continuity across departments and over time.
Even simple shared notes reduce information loss during transitions.
For patients living far away, tele-follow-ups can maintain engagement and catch problems early.
Doctors who use these tools wisely reduce unnecessary delays.
Over time, data from trauma amputees can reveal patterns and guide better protocols.
Continuous improvement depends on learning from real outcomes.
Trauma care, recovery, and prosthetic use are one continuous journey.
Doctors who see the full path make better decisions at every stage.
Life-saving care and functional planning are not opposites. They can coexist.
Early attention to function multiplies the value of survival.
Small actions taken early prevent large problems later.
Doctors shape not just survival, but the quality of life that follows.
Trauma amputees do best when care is structured, humane, and forward-looking.
Clear ICU-to-prosthesis pathways turn uncertainty into direction.
For many clinicians, the surgery is only the first step. What happens after the operation

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body

Age changes the body, but it does not take away the need for independence, dignity,