
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


A prosthetic device does not work through muscles alone. It works through the brain. Every step, grip, and adjustment depends on attention, memory, judgment, and learning. When cognitive function is reduced, even a well-designed prosthetic can become unsafe or unusable. For doctors involved in amputee care, understanding cognition is just as important as understanding strength or balance.
At Robobionics, we have seen many cases where physical recovery looked promising, but prosthetic use failed because cognitive challenges were missed early. Some patients struggled to remember safety steps. Others found it hard to learn movement patterns or recognize risk. These issues are not always obvious during short clinical visits, yet they strongly affect outcomes.
This article focuses on cognitive function and prosthetic use, with a clear emphasis on screening tools that doctors can use in daily practice. It explains why cognition matters, how different cognitive domains affect prosthetic safety, and which simple screening methods help guide better decisions. The goal is not to exclude patients, but to match prosthetic plans to real-world ability.
If you are a doctor, rehabilitation specialist, or part of an amputee care team, this guide will help you identify cognitive risks early and act on them wisely. When cognition is assessed with care and respect, prosthetic outcomes become safer, more predictable, and more humane.
Using a prosthetic is not an automatic physical action.
Every movement requires planning, attention, and constant adjustment based on feedback from the body and the environment.
The brain decides when to shift weight, how fast to move, and how to respond if balance feels unstable.
Even simple activities like standing up or turning require active thinking during early prosthetic use.
If cognitive function is limited, these tasks become unsafe very quickly.
This is why physical strength alone never predicts prosthetic success.
Prosthetic use creates ongoing mental demand.
Patients must monitor socket comfort, ground surface, fatigue, and surrounding obstacles at the same time.
This mental load increases further in unfamiliar or crowded environments.
When cognitive reserve is low, patients tire mentally before they tire physically.
This leads to poor judgment, delayed reactions, and unsafe decisions.
Doctors must recognize this early to prevent falls and injuries.
When cognition is not assessed, prosthetic failure is often blamed on motivation or attitude.
In reality, many patients simply cannot process the required information fast enough.
This misunderstanding leads to frustration for both patients and clinicians.
Ignoring cognition increases fall risk, device abandonment, and emotional distress.
It also wastes rehabilitation time and resources.
Early screening protects outcomes and patient dignity.
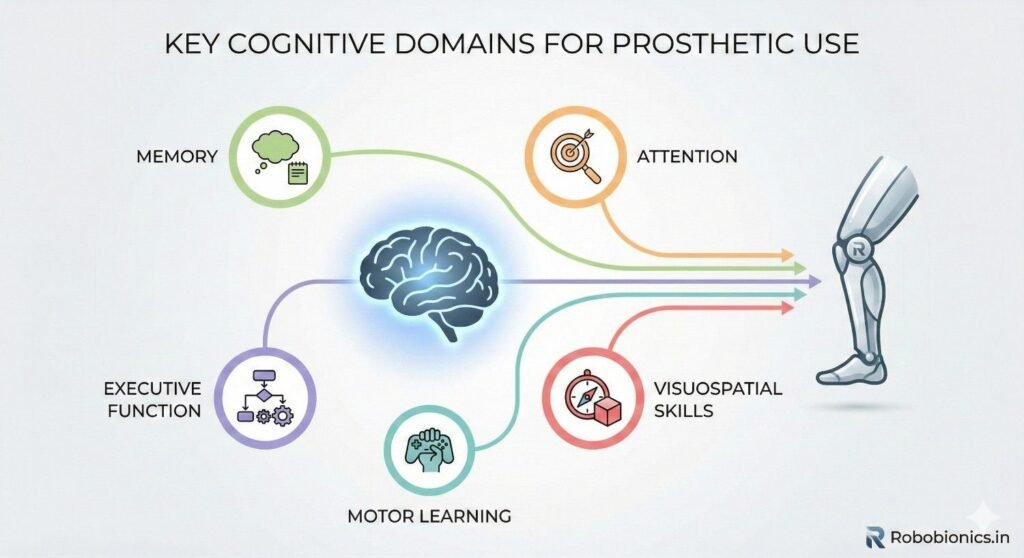
Attention allows a patient to focus on walking, standing, or using a prosthetic hand without distraction.
Prosthetic training demands sustained focus, especially in early stages.
Poor attention leads to missed steps and delayed responses.
Patients with attention difficulties may perform well briefly, then deteriorate suddenly.
This inconsistency is dangerous during mobility tasks.
Doctors should always observe how long focus can be maintained.
Learning to use a prosthetic requires remembering repeated instructions.
Patients must recall safety steps, movement patterns, and daily care routines.
Memory issues disrupt this learning process.
If instructions are forgotten between sessions, progress stalls.
Repeated errors increase risk and reduce confidence.
Memory screening helps set realistic training plans.
Executive function governs planning, decision-making, and risk awareness.
It helps patients judge when to rest, when to stop, and when a situation is unsafe.
This domain is critical for independent prosthetic use.
Poor judgment leads to risky behavior, such as walking when fatigued or ignoring pain signals.
These patients may overestimate their ability.
Doctors must identify this risk early.
Processing speed affects how quickly a patient responds to imbalance or obstacles.
Prosthetic users must react promptly to prevent falls.
Slow processing increases accident risk.
Older adults and patients with neurological conditions often show delayed reactions.
This does not always appear during conversation.
Functional testing reveals these delays more clearly.
Normal aging affects memory, attention, and processing speed.
Even mild age-related changes can impact prosthetic learning.
This is especially relevant in geriatric amputees.
Age-related decline does not mean prosthetic use is impossible.
It means planning must be adjusted.
Screening helps tailor safe expectations.
Stroke, head injury, and neurodegenerative diseases are common in amputee populations.
These conditions directly affect cognition and motor control.
Their impact may fluctuate daily.
Patients may appear clear during assessment but struggle later.
Fatigue often worsens cognitive performance.
Repeated evaluation is sometimes necessary.
Conditions such as diabetes, kidney disease, and infections affect brain function.
Poor sleep, pain, and medications also reduce clarity.
These factors are often temporary but significant.
Doctors must consider reversible causes of cognitive change.
Treating the underlying issue can improve prosthetic readiness.
Screening helps detect when delay is safer.
Cognitive screening should happen before selecting a prosthetic design.
This ensures device complexity matches learning capacity.
Early screening prevents costly mismatches.
Doctors should not wait for rehabilitation failure to assess cognition.
Prevention is always safer than correction.
This step protects both patient and clinic outcomes.
Cognition influences how fast and how far training can progress.
Patients with limited cognitive reserve need shorter sessions and more repetition.
Training pace must match learning ability.
Screening during planning helps therapists structure sessions realistically.
It reduces frustration and unsafe pressure.
Progress becomes more predictable.
When physical healing is adequate but progress remains slow, cognition should be reassessed.
This is often missed in busy clinical settings.
Poor progress is a signal, not a failure.
Reassessment helps identify hidden barriers.
Plans can then be adjusted without blame.
This improves trust and engagement.
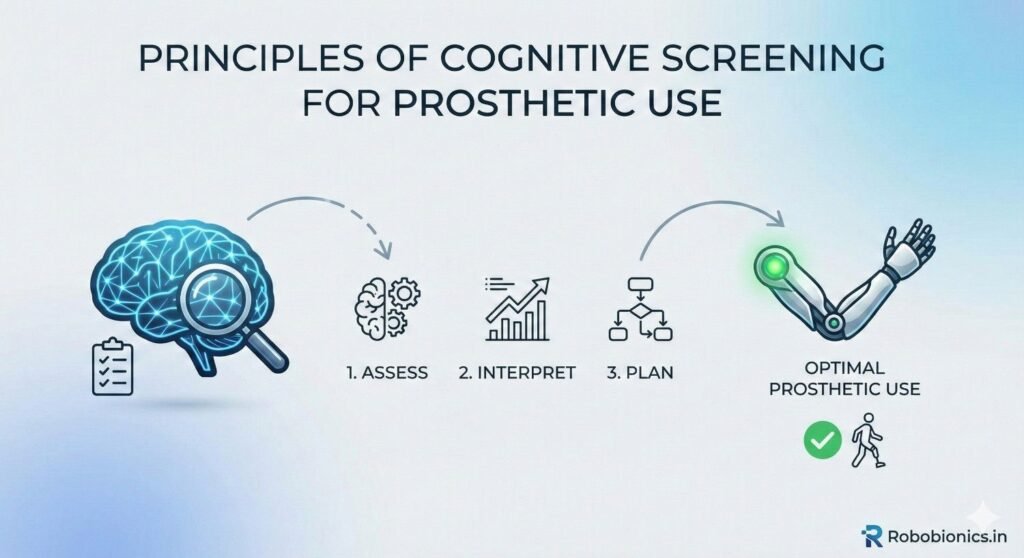
Cognitive screening does not label or diagnose patients.
It identifies risk and guides planning.
This distinction must be clear to patients.
Doctors should explain screening as a safety step.
Transparency reduces fear and stigma.
Respectful framing encourages cooperation.
Screening does not require complex neuropsychological testing.
Simple, validated tools provide valuable insight.
They fit easily into clinical workflows.
The goal is practical decision-making.
Doctors need usable information, not academic detail.
Efficiency improves adoption.
Scores alone do not tell the full story.
How a patient responds, hesitates, or asks for clarification matters greatly.
Observation adds depth to results.
Doctors should combine scores with functional insight.
This leads to better decisions.
Clinical judgment remains central.
The Mini-Cog is fast and simple.
It assesses memory and basic executive function in a few minutes.
This makes it suitable for busy clinics.
Patients are asked to recall words and draw a clock.
Difficulty suggests further evaluation is needed.
It works well as an initial filter.
The Montreal Cognitive Assessment provides broader coverage.
It looks at attention, memory, language, and executive function.
This depth is useful for prosthetic decisions.
It takes longer but offers clearer insight.
Doctors often use it when risk is suspected.
Results guide device complexity and training intensity.
The Mini-Mental State Examination is widely known.
It assesses orientation and basic memory.
However, it may miss subtle deficits.
Patients may score well yet struggle with real-world tasks.
This limits its value in prosthetic planning.
Doctors should interpret results cautiously.
How a patient follows instructions reveals cognitive function.
Repeated clarification requests or skipped steps are important signals.
These observations often matter more than test scores.
Doctors should note consistency and confidence.
Confusion under mild stress is a red flag.
Real-world learning mirrors training demands.
Prosthetic use often requires doing two things at once.
Walking while talking or turning while scanning the environment is common.
Dual-task ability reflects cognitive reserve.
Simple tests can reveal difficulty.
Patients who freeze or slow down significantly need caution.
This predicts fall risk.
Cognition may worsen as patients tire.
Short assessments may miss this effect.
Longer observation provides better insight.
Doctors should watch for decline near session end.
This helps plan safe training limits.
Fatigue management becomes part of care.
Cognitive screening results must be explained gently.
Language should focus on safety and support.
Avoid terms that imply failure or inability.
Patients respond better when risks are framed practically.
This builds trust and acceptance.
Honest communication prevents misunderstanding.
Caregivers often support prosthetic use daily.
They should understand cognitive risks and needs.
Their involvement improves safety.
Doctors should share guidance with consent.
This helps align expectations.
Support systems become more effective.
Goals must match what the patient can manage consistently.
This may mean slower progress or simpler devices.
Matching goals prevents frustration.
Patients appreciate realistic planning.
Success feels achievable rather than forced.
Cognition-aware goals improve long-term use.
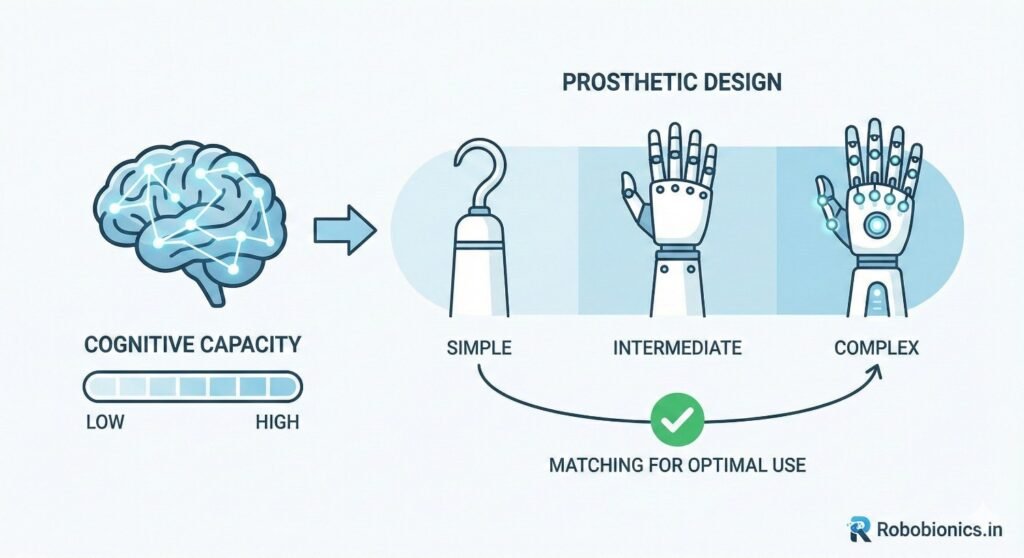
Prosthetic devices vary greatly in how much thinking they demand from the user.
Some require constant attention to position, timing, and control, while others behave in more predictable ways.
For patients with reduced cognitive reserve, simpler designs reduce mental strain and improve safety.
A simple prosthetic allows the brain to focus on balance and environment rather than device control.
This lowers fall risk and fatigue during daily use.
Doctors should always consider cognitive effort as part of device selection.
Advanced prosthetic components may offer benefits, but they also increase learning demand.
Multiple modes, sensors, or adaptive responses can confuse patients with slower processing speed.
What looks helpful in theory may overwhelm in practice.
Patients with good physical ability may still struggle cognitively with complex systems.
This mismatch often leads to anxiety and inconsistent use.
Cognitive screening helps doctors decide when advanced technology is appropriate.
Predictable prosthetic behavior supports cognitive confidence.
When a device responds the same way each time, learning becomes easier.
Unpredictable feedback increases hesitation and fear.
Patients with mild cognitive impairment rely heavily on routine.
Consistency allows habits to form safely.
Doctors should prioritize predictable designs for long-term success.
Training sessions should match the patient’s attention span and learning speed.
Long sessions may exhaust cognitive resources before physical ones.
Shorter, focused sessions often produce better results.
Doctors and therapists should plan training in manageable blocks.
Frequent breaks protect attention and reduce errors.
This approach improves retention and confidence.
Repetition is essential for patients with memory challenges.
Repeating the same sequence helps convert conscious effort into habit.
This reduces cognitive demand over time.
Training should follow a consistent structure each session.
Routine supports recall and reduces anxiety.
Predictability enhances learning efficiency.
Clear cues support patients who struggle with memory or attention.
Simple verbal prompts and visual markers guide safe movement.
These cues reduce reliance on internal recall.
Doctors should encourage therapists to use consistent language.
Changing terms can confuse learning.
Consistency strengthens understanding and safety.
Some patients show poor judgment and overestimate their ability.
They may insist on independence before it is safe.
This behavior is linked to executive function deficits.
Doctors should not rely solely on patient self-report.
Objective observation is essential.
Overconfidence increases injury risk.
Large day-to-day variation often signals cognitive fatigue or impairment.
Patients may perform well one day and poorly the next.
This unpredictability affects safety.
Doctors should look for patterns rather than isolated success.
Consistency matters more than peak performance.
Screening helps explain variability.
Patients with cognitive impairment may repeat the same mistakes.
They struggle to apply corrections even after explanation.
This slows progress and increases risk.
This pattern should prompt reassessment.
More support or simpler goals may be needed.
Ignoring it leads to frustration.
Lower limb prosthetic use places high cognitive demand on balance and navigation.
Patients must constantly scan the environment and adjust movement.
This requires attention and quick decision-making.
Cognitive screening is especially critical in these cases.
Even mild impairment can increase fall risk.
Doctors should be cautious and thorough.
Upper limb prosthetics rely more on planning and coordination.
Tasks such as grasping or switching grips require sequencing.
Memory and attention play a major role.
Patients may appear functional at rest but struggle during tasks.
Observation during simulated activities helps.
Cognitive screening guides device choice and training pace.
Bilateral amputees face even higher cognitive demand.
They must relearn many daily tasks simultaneously.
This can overwhelm limited cognitive reserve.
Screening is essential before aggressive prosthetic goals.
Progress must be staged carefully.
Safety and emotional health depend on realistic planning.
Caregivers often help reinforce routines and safety steps.
They remind patients of wear schedules and precautions.
This support compensates for memory gaps.
Doctors should involve caregivers early.
Education improves consistency at home.
Shared understanding reduces risk.
Cognition can change due to illness, medication, or aging.
Caregivers often notice subtle shifts first.
Their observations are valuable.
Doctors should encourage regular feedback.
Early detection allows timely adjustment.
This prevents accidents and setbacks.
While support is important, overdependence can reduce confidence.
Patients should be encouraged to do what they can safely.
Balance is key.
Doctors should guide caregivers on appropriate assistance.
This promotes independence within limits.
Healthy support improves outcomes.
Cognitive screening can create anxiety if poorly explained.
Patients may fear loss of independence.
Doctors must address this sensitively.
Screening should be framed as a safety measure.
It protects patients rather than judging them.
Clear communication reduces resistance.
Cognitive impairment should not automatically exclude prosthetic use.
It guides adaptation and support level.
Many patients succeed with the right plan.
Doctors should emphasize possibilities, not limits.
This maintains dignity and motivation.
Ethical care is inclusive and realistic.
Cognition is not static.
Improvement or decline may occur.
Decisions should be revisited periodically.
Doctors should plan reassessment points.
Flexibility improves long-term care.
Static decisions rarely serve patients well.
Cognitive screening works best when it is routine.
This normalizes the process and reduces stigma.
Short tools fit easily into assessments.
Doctors should select tools that match clinic flow.
Consistency improves reliability.
Routine use improves outcomes.
All team members should understand cognitive impact.
Training helps staff recognize early signs.
Shared awareness improves coordination.
Doctors play a key role in leading this culture.
Education strengthens team confidence.
Better screening leads to safer care.
Screening results must inform decisions.
Documentation ensures continuity across teams.
Ignoring results defeats the purpose.
Doctors should link findings to action plans.
This closes the loop.
Effective follow-through protects patients.

As amputee populations age, cognitive issues will increase.
Prosthetic care must adapt to this reality.
Early screening will become standard practice.
Doctors who adopt this approach early are better prepared.
Cognitive-aware care improves safety and satisfaction.
It reflects modern, humane medicine.
Manufacturers can design devices with cognitive simplicity in mind.
Clear feedback, stable behavior, and easy maintenance support users.
Design choices influence cognitive load.
At Robobionics, we see this as a shared responsibility.
Technology should support the brain, not burden it.
Design must continue to evolve with user needs.
Cognitive function shapes every aspect of prosthetic use.
When doctors screen early and act wisely, outcomes improve.
Patients feel safer, more confident, and more respected.
Cognition-aware prosthetic care is not an extra step.
It is a core part of good medicine.
When the brain is supported, the body can follow.
Cognitive function plays a quiet but powerful role in prosthetic success. A patient may have good strength and healing, yet still struggle if attention, memory, or judgment are reduced. When doctors recognize this early, prosthetic care becomes safer, more predictable, and far more humane.
Screening tools do not exist to limit patients. They exist to guide better decisions. Simple cognitive assessments help doctors choose the right device, set realistic goals, and design training that patients can actually manage in daily life. This prevents falls, frustration, and early prosthetic abandonment.
At Robobionics, our experience has shown that cognition-aware prosthetic planning leads to better long-term use and higher patient confidence. When the brain is respected as much as the body, prosthetic technology becomes a true support rather than a risk. Cognitive screening, when used with care and clarity, strengthens outcomes for patients, families, and care teams alike.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body