
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation



The success of a prosthetic does not begin on the day it is fitted. It begins much earlier, often in the first few days after amputation. What happens during this early phase quietly shapes every future outcome. Comfort, function, long-term use, and even patient confidence are all influenced by post-amputation care decisions made by doctors.
At Robobionics, after working closely with surgeons, rehabilitation teams, and thousands of amputees across India, we have seen a clear pattern. Patients who receive structured, thoughtful post-amputation care adapt to prosthetics faster and use them more consistently. Those who do not often struggle, no matter how advanced the prosthetic is.
This article is written for medical doctors who want to improve prosthetic outcomes through better post-amputation care. It focuses on practical protocols, timing decisions, and patient guidance that truly matter in real life. These are not textbook ideals. They are field-tested insights shaped by Indian patients, homes, and healthcare realities.
Post-amputation care is often treated as a recovery phase that simply needs to pass. In reality, it is an active preparation phase for prosthetic use. Decisions made here affect comfort, healing quality, and long-term function.
When this phase is rushed or poorly guided, even the best prosthetic struggles to perform well.
Patients who receive structured care early develop healthier residual limbs and better movement patterns. These patients adapt to prosthetics with less pain and fear.
Poor early care leads to stiffness, skin issues, and emotional resistance that are hard to reverse later.
Surgeons and physicians guide early expectations, movement, and healing protocols. Their words and instructions shape patient behavior during the most sensitive phase.
Clear guidance from MDs builds trust and sets the tone for rehabilitation.

The first goal after amputation is protection. Wound care, infection prevention, and edema control must be consistent and gentle.
Overhandling or neglect during this stage can compromise future prosthetic fitting.
Pain control should allow movement, not eliminate sensation completely. Excessive immobilization delays recovery and increases stiffness.
Balanced pain management supports healing while encouraging early engagement.
Improper positioning causes contractures that limit prosthetic use later. Simple positioning advice prevents long-term restrictions.
Doctors must reinforce correct positioning repeatedly, not just once.
A well-shaped residual limb fits better into a prosthetic socket. Poor shape leads to pressure points and discomfort.
Edema control is not cosmetic. It is functional preparation.
Gentle compression supports circulation and reduces swelling. Timing and technique matter greatly.
MDs should guide patients clearly on when and how compression is safe.
Limb volume changes rapidly in early weeks. Regular review prevents surprises during prosthetic fitting.
Ignoring these changes delays readiness.
After amputation, the skin takes on new mechanical stress. It must be healthy and resilient.
Fragile skin increases pain and reduces wear time.
Cleanliness, moisture balance, and inspection routines protect skin health.
Doctors should educate patients and caregivers on simple daily checks.
Gentle touch and exposure reduce hypersensitivity over time. Avoiding the limb increases fear and discomfort.
Early desensitization improves tolerance during prosthetic training.
Immobilization weakens muscles quickly. Even small movements preserve strength.
Doctors should encourage safe activity as early as possible.
Stiff joints limit prosthetic alignment and comfort. Once lost, range is difficult to regain.
Daily guided movement protects future mobility.
Patients often adopt poor movement habits to avoid pain. These habits persist into prosthetic use.
Early correction prevents long-term inefficiency.
Amputation is a major emotional event. Patients experience shock, sadness, or anger.
Ignoring this emotional state slows physical recovery.
Words shape hope and fear. Clear, calm, and realistic language reassures patients.
Avoiding extremes protects emotional balance.
Introducing prosthetics early as a future tool builds direction. This should be done gently, not as pressure.
Early vision supports engagement.
Patients often imagine recovery as linear. Explaining ups and downs prevents panic.
Understanding the process improves cooperation.
Patients should feel involved, not passive. Simple self-care tasks build confidence.
Active roles improve outcomes.
Families influence recovery strongly. Early education prevents unrealistic pressure.
Doctors should involve families in conversations.
Gaps between surgery and rehabilitation delay progress. Clear handovers prevent confusion.
MDs play a key role in continuity.
Details about incision type, healing concerns, and limb sensitivity matter for prosthetic planning.
Clear documentation improves collaboration.
Too early referrals overwhelm patients. Too late referrals waste time.
Balanced timing supports smooth transition.
Persistent swelling, extreme pain, or fear of touch signal future difficulties.
Early identification allows early correction.
Avoidance, withdrawal, or unrealistic expectations require attention.
These signs predict adaptation challenges.
Protocols should adapt to patient response, not remain rigid.
Flexibility improves outcomes.
The period after initial healing is where long-term patterns are set. Patients begin to test their limits, and habits start to form quietly.
Care during this phase determines whether the residual limb becomes prosthetic-ready or develops avoidable barriers.
Once wounds are stable, the focus must shift toward preparing for function. This includes movement quality, skin tolerance, and emotional confidence.
MDs should clearly explain this shift so patients understand why care routines change.
Patients often feel safer limiting movement during this phase. While understandable, prolonged caution leads to stiffness and weakness.
Doctors must gently guide patients out of this comfort zone.
Pain after amputation is not uniform. Surgical pain, nerve pain, and phantom sensations all behave differently.
Clear identification helps tailor treatment without over-restricting activity.
Medication helps early recovery, but long-term reliance reduces activity and awareness.
Gradual reduction paired with movement builds confidence and resilience.
Not all discomfort is harmful. Patients need help distinguishing warning pain from adaptation discomfort.
This understanding prevents unnecessary avoidance.
Scars that are tight or sensitive interfere with socket comfort. Poor scar mobility leads to pressure pain later.
Scar care is not cosmetic. It is functional.
Once healed, gentle movement around the scar improves flexibility and sensation.
MD guidance ensures safety and consistency.
Scar sensitivity can increase or decrease unpredictably. Regular review helps adjust care plans.
Ignoring this stage causes future fitting delays.
Strength should support daily tasks, not just exercise goals.
Doctors should align strengthening with future prosthetic use.
Amputation affects the whole body. Core strength and opposite limb health matter greatly.
Neglect here leads to imbalance and fatigue.
Patients often overload the intact limb. Early guidance prevents secondary injuries.
Balanced care protects long-term mobility.
The residual limb must learn to accept pressure safely.
This process must be slow, guided, and monitored.
Skin tolerance develops through controlled exposure.
Avoiding all pressure delays readiness.
Redness that fades is normal. Persistent pain is not.
Teaching this difference empowers patients.
Early recovery is about survival. Subacute care is about adaptation.
Patients need support to make this mental shift.
Many patients fear that prosthetics will hurt or fail.
MDs should address these fears honestly and early.
Questions during this phase are signs of engagement.
Open answers prevent misinformation.
Referral timing should follow readiness, not fixed dates.
Every patient heals differently.
Early referrals without readiness create frustration.
Doctors must manage expectations carefully.
Early communication with prosthetists improves planning.
This teamwork reduces delays later.
Healing quality affects skin strength and energy levels.
Poor nutrition slows readiness.
Protein, hydration, and micronutrients matter.
Doctors should address basics before advanced care.
Nutrition advice should be practical and respectful.
Small improvements make real differences.
Isolation slows recovery. Safe social interaction builds confidence.
Doctors should encourage gradual engagement.
Patients worry about returning to work early.
Honest discussions reduce anxiety.
Recovery plans must fit the patient’s actual life.
This alignment improves adherence.
Recovery is uneven. One bad day does not signal failure.
MDs should track trends over time.
Rigid protocols ignore human variation.
Flexibility improves outcomes.
Acknowledging small gains sustains motivation.
This encouragement matters deeply.
Many delays in prosthetic success are blamed on healing time. In reality, poor conditioning is often the real cause. A limb may be healed but not prepared.
Pre-prosthetic conditioning builds the physical and mental base needed for smooth fitting and training.
Conditioning is often left to therapists alone. However, MD guidance gives it medical weight and urgency.
When doctors reinforce conditioning goals, patients take them more seriously.
Prosthetic use is a full-body activity. Balance, posture, and endurance matter as much as the residual limb.
MDs should encourage whole-body readiness, not isolated focus.
The skin should tolerate touch, pressure, and daily movement without breakdown. Persistent sensitivity signals delayed readiness.
Doctors should check skin response patterns, not just appearance.
Rapid volume changes make socket fitting difficult. Some fluctuation is normal, but trends matter.
Stable volume supports better early prosthetic comfort.
Joint stiffness limits alignment options. Even small losses affect comfort and gait later.
MDs should confirm functional range, not just passive range.
Strength should support standing, transfers, and sustained activity.
Isolated muscle power without functional endurance leads to fatigue.
Fear of imbalance reduces prosthetic trust. Balance confidence must be built before fitting.
Doctors should assess balance behavior, not just test scores.
Prosthetic use increases energy demand. Poor endurance limits wear time.
Basic endurance readiness improves early success.
Patients must understand that prosthetics feel unfamiliar at first. Early discomfort does not mean failure.
MDs should reinforce this message clearly.
Readiness includes willingness to engage in daily practice.
Doctors should assess readiness through conversation, not assumption.
Severe anxiety or depression delays learning.
Addressing mental health early protects outcomes.
Medical clearance without functional readiness leads to poor first experiences.
Doctors should align clearance with preparation, not pressure.
Skipping discussions about effort, fatigue, or limits creates future disappointment.
Honest conversations protect trust.
Referral is not the end of care. Ongoing MD involvement matters.
Disengagement creates gaps.
Using shared terms and goals reduces confusion for patients.
MDs can lead this alignment.
Details about skin sensitivity, pain patterns, and fears help prosthetists plan better.
Clear notes save time and frustration.
MD follow-up during prosthetic training catches issues early.
This oversight improves long-term use.
Small skin issues should not halt progress completely.
Guided adjustments often solve problems.
Pain needs evaluation, not immediate retreat.
Doctors should guide measured responses.
Overreaction to minor setbacks scares patients.
Calm guidance preserves confidence.
The first fitting is a learning experience, not a test.
MDs should set this expectation clearly.
Early awkwardness is normal. Improvement comes with time.
Patience reduces abandonment risk.
Patients should know help is available.
This reassurance encourages honesty.
The first three months after prosthetic fitting decide whether the device becomes part of daily life or slowly gets abandoned. This period is when habits form and doubts appear.
MD involvement during this window reassures patients and prevents small issues from becoming permanent barriers.
Patients often want to progress quickly once they receive a prosthetic. While enthusiasm is helpful, rushing increases pain and disappointment.
Doctors should clearly guide pacing and remind patients that slow progress is normal and safer.
Early discomfort is expected, but pain should never be dismissed. MDs help patients understand which sensations are part of adaptation and which need attention.
This clarity prevents both fear and neglect.
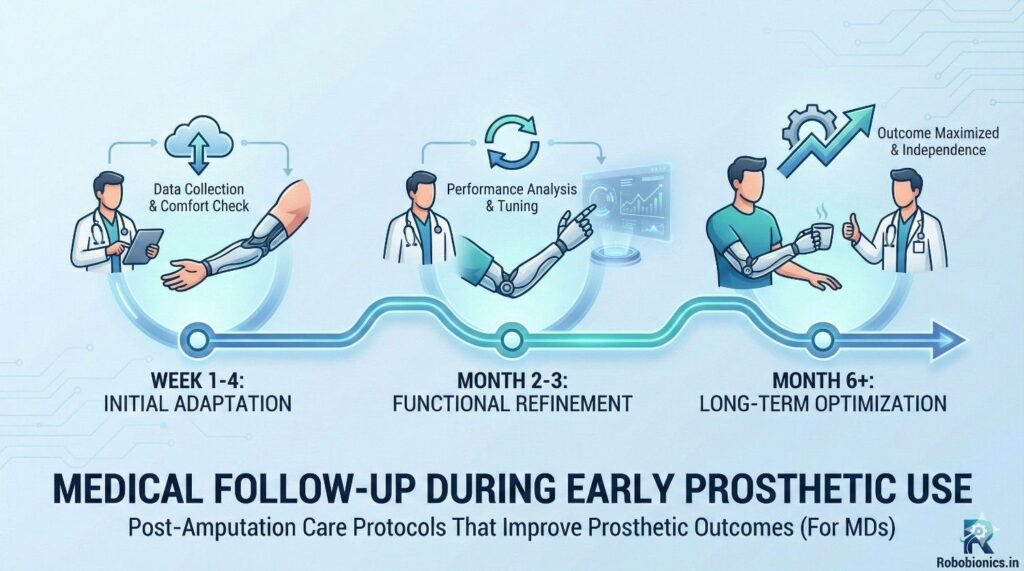
Follow-ups should not be routine formalities. Each visit should have a clear purpose, such as skin review, pain mapping, or endurance assessment.
Purposeful visits improve patient confidence and clinician insight.
How long did you wear the prosthetic each day is more useful than are you using it regularly.
Specific questions reveal real usage patterns and hidden struggles.
Patients may underreport issues. Simple observation of standing, walking, or hand use reveals more than words alone.
MDs should rely on both observation and conversation.
Redness that fades within minutes is common. Persistent redness or sharp pain is not.
Doctors must teach patients this difference repeatedly.
Many patients stop using prosthetics after one skin issue. Fear grows quickly.
Calm reassurance and clear action plans prevent long-term avoidance.
Early issues often need quick prosthetic adjustments, not medical pauses.
MDs should coordinate closely with prosthetists to keep momentum.
Muscle soreness and pressure discomfort are expected early on. Nerve pain or deep joint pain is not.
Clear differentiation prevents unnecessary stoppage.
Stopping use at the first sign of discomfort delays adaptation.
Doctors should guide measured responses instead of blanket restrictions.
Patients often hide pain to avoid being told to stop.
A non-judgmental approach encourages honesty.
Fatigue is one of the most common early complaints. Patients often interpret it as failure.
Doctors must explain that increased energy use is normal during adaptation.
Short, planned wear sessions build endurance better than long, exhausting attempts.
MD guidance on pacing improves long-term tolerance.
Anemia, poor sleep, or nutrition issues worsen fatigue.
MDs should rule out these contributors early.
Awkward movements and slow progress frustrate patients.
Doctors should normalize these feelings and remind patients of the learning curve.
Patients often compare themselves with online stories or peers.
MDs should gently redirect focus to individual progress.
Using a prosthetic changes how patients see themselves.
Acknowledging this shift supports emotional adaptation.
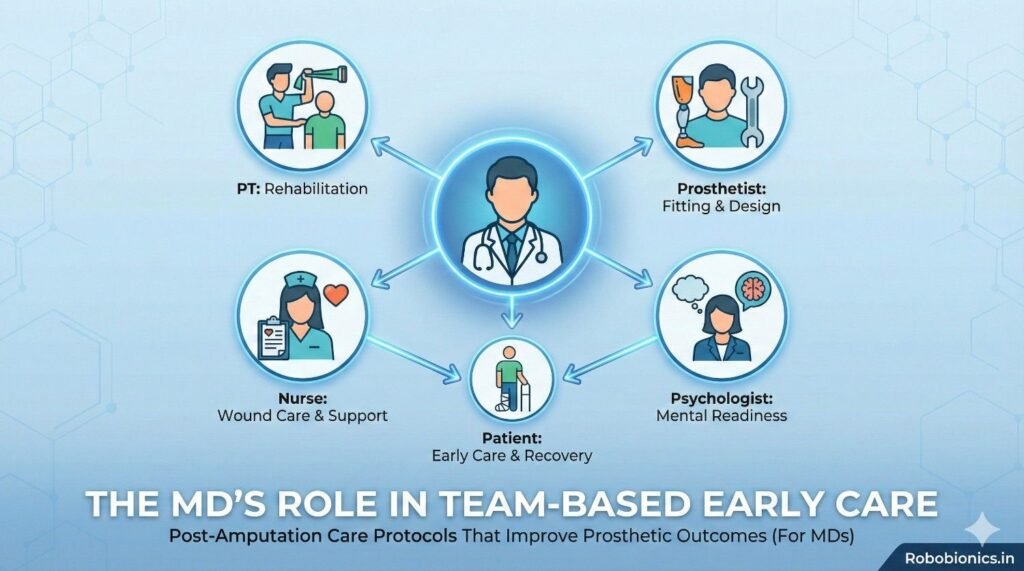
During early use, patients interact with many professionals. MDs act as the anchor who provides continuity.
This role builds trust and reduces confusion.
When MDs reinforce therapist and prosthetist advice, patients follow it more closely.
Unified messaging improves adherence.
MDs help decide when an issue needs medical intervention versus adjustment or time.
This judgment prevents unnecessary disruption.
Skipping appointments, reduced wear time, or vague complaints often signal trouble.
Early recognition allows timely support.
Fear grows faster than pain. One bad experience can change behavior.
MDs should address fear directly, not indirectly.
Patients should feel safe saying they are struggling.
This openness prevents silent abandonment.
Initial goals may prove unrealistic. Adjusting them early protects motivation.
Doctors should guide goal revision without framing it as failure.
Early goals should focus on basic function and comfort.
Refinement comes later.
Progress often feels invisible to patients.
MDs should point out improvements clearly.
Many prosthetic failures happen months or years after a good start. This usually occurs when medical follow-up fades and small issues go unnoticed.
Long-term outcomes improve when MDs stay involved beyond the initial success phase.
Early care is hands-on and directive. Long-term care should shift toward support and guidance.
MDs help patients adapt prosthetic use as life, work, and health change.
Bodies change. Weight fluctuates. Work demands evolve. Prosthetic care must adjust with these changes.
Doctors should expect change, not stability.
Skin tolerance can decrease due to friction, sweat, or volume changes.
Regular skin checks prevent sudden breakdowns that lead to abandonment.
Long-term prosthetic use affects joints and spine. Poor alignment or overuse leads to pain.
MDs should monitor posture, gait, and secondary strain.
Patients often overload the intact limb for years without noticing.
Early detection prevents long-term disability.
Once patients appear functional, follow-up often stops. This creates a care gap.
MDs should schedule periodic reviews even when things seem stable.
Job changes, travel, or aging alter prosthetic needs.
Discussing these changes early prevents mismatch.
Small proactive adjustments prevent major problems.
Doctors should promote prevention, not crisis response.
A patient’s relationship with their prosthetic evolves. Initial acceptance may later turn into frustration or fatigue.
MDs should allow space for these shifts.
Daily prosthetic use requires effort. Burnout is real.
Doctors can normalize rest, breaks, and reassessment without framing it as failure.
Long-term use is sustained by purpose, not excitement.
MDs should reconnect patients to personal goals, not performance metrics.
Late pain does not always mean prosthetic failure. It may signal alignment changes or health shifts.
Calm evaluation prevents unnecessary abandonment.
Some issues need rest. Others need continued use with adjustment.
MD judgment is key to this balance.
Stopping prosthetic use completely often worsens outcomes.
Gradual modification protects function.
Patients who know they can return without judgment are more honest.
Trust improves early reporting of issues.
Patients should learn to manage their prosthetic health over time.
MDs act as mentors, not controllers.
Aging changes strength, balance, and endurance.
Early planning prevents sudden decline.
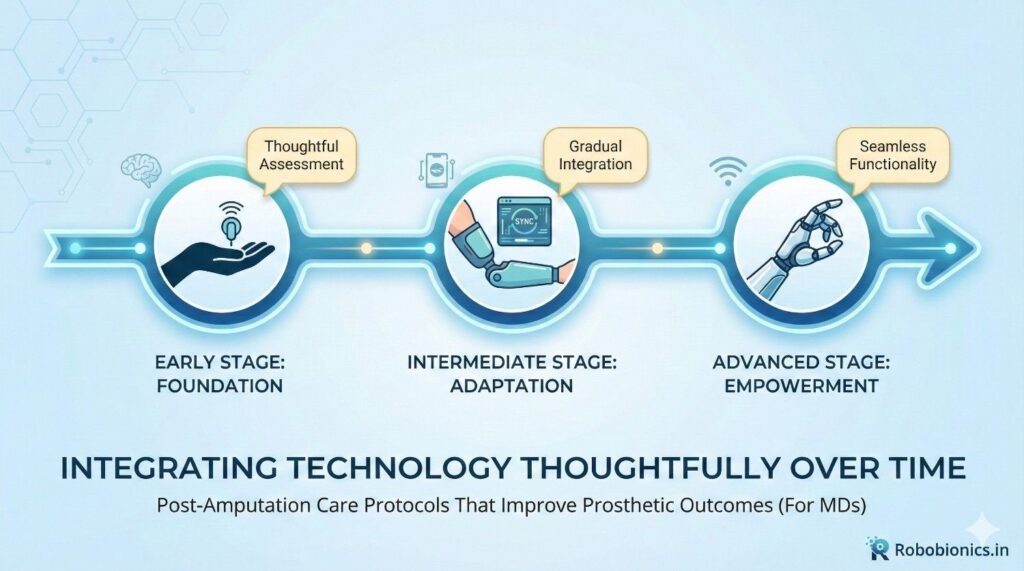
Technology can help, but it cannot replace medical oversight.
MDs must guide upgrades carefully.
Newer is not always better. Unnecessary upgrades increase risk.
Decisions should follow need, not novelty.
Technology choices should align with current life demands.
This alignment improves satisfaction.
At Robobionics, we design prosthetics that tolerate real Indian conditions, long wear, and evolving needs.
Durability supports long-term confidence.
We believe MDs are central to prosthetic success.
Our care models encourage ongoing collaboration.
We learn from patient journeys over years, not weeks.
This learning improves future care.
Prosthetic success is often discussed as a matter of technology, fit, or training. While these factors matter, they sit on a much deeper foundation. That foundation is post-amputation care. The choices made by medical doctors in the days, weeks, and months after amputation quietly decide whether a prosthetic will become a useful part of life or a difficult burden.
Post-amputation care is not a waiting period. It is an active phase of preparation. Every instruction about positioning, movement, skin care, and pain shapes how the body heals and how the mind adapts. When this phase is handled with clarity and purpose, patients arrive at prosthetic fitting ready, confident, and realistic. When it is rushed or vague, even advanced prosthetics struggle to succeed.
For MDs, this responsibility is both clinical and human. Patients often look to doctors not just for treatment, but for reassurance and direction. The language used, the expectations set, and the time taken to explain the recovery journey all influence patient behavior. Calm, honest guidance reduces fear. Clear timelines prevent unrealistic hope. Gentle encouragement promotes active participation instead of passive waiting.
The weeks following surgery are especially powerful. Proper edema control, positioning, and early movement protect future mobility. Skin care and desensitization build tolerance for socket use. Strength and range of motion preserve alignment options. Emotional support during this phase prevents withdrawal and avoidance. None of these steps are complex, but they require consistency and reinforcement from doctors.
As recovery moves into the subacute and pre-prosthetic phases, MDs play a critical role in shifting focus from healing to readiness. This transition must be explained clearly to patients and families. Conditioning, endurance, and mental preparation become just as important as wound closure. Declaring readiness too early creates false starts. Declaring it too late creates frustration. Medical judgment grounded in function, not calendars, protects outcomes.
The first 90 days of prosthetic use represent another fragile window. Habits form quickly, both good and bad. Medical follow-up during this period reassures patients, clarifies discomfort, and prevents fear from taking root. When MDs remain involved, patients are less likely to silently struggle or abandon use. Small interventions during this phase often decide long-term success.
Long-term care is where prosthetic outcomes are truly secured. Bodies change. Lives change. Prosthetic needs evolve. Without ongoing medical oversight, patients adapt poorly or disengage slowly. Periodic review, preventive guidance, and psychological support sustain use over years, not just months. Prosthetic success should be measured by sustained comfort and participation in life, not by early milestones alone.
At Robobionics, our experience across India has shown us that prosthetic outcomes improve dramatically when MDs view post-amputation care as a continuum, not a handover. When surgeons, physicians, rehabilitation teams, and prosthetists work in alignment, patients feel supported rather than passed along. This continuity builds trust, reduces failure, and restores dignity.
Post-amputation care is not about doing more. It is about doing the right things at the right time, with the right mindset. It respects the body’s pace, the patient’s emotions, and the realities of daily life. When MDs lead this process with clarity and compassion, prosthetics stop being medical devices and start becoming tools for living.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body