
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation



Nutrition is often treated as a side note before prosthetic fitting. In reality, it decides how well the body heals, how strong the residual limb becomes, and how soon a patient is ready for a prosthesis. A well-designed prosthetic can only work as well as the body wearing it. Without proper nutrition, even the best rehabilitation plan slows down.
For medical teams, nutrition before prosthesis is not about weight alone. It is about tissue strength, skin health, muscle recovery, and energy levels. Protein intake, calorie balance, and simple nutrient timing directly affect wound healing, pain levels, and limb tolerance.
This guide is written for doctors and medical teams who want clear, practical nutrition targets that support early and successful prosthetic use. It avoids complex diet theory and focuses on what actually helps patients heal faster, adapt better, and move forward with confidence.
After an amputation, the body enters a high-demand healing state. Tissues are repairing, muscles are adjusting, and the immune system is active every day. All of this needs fuel. If calories and protein are low, healing slows down even if surgery and wound care are perfect. Wounds stay fragile, swelling lasts longer, and the residual limb remains sensitive. This directly delays prosthetic trials because the limb is simply not ready to tolerate load or socket contact.
From a medical point of view, this delay often looks like a surgical or rehab issue. In reality, it is very often a nutrition gap. Patients may look stable on the outside but lack the building blocks needed for recovery. Identifying this early saves weeks of delay later.
Every patient loses some muscle after surgery. This is normal. The problem starts when nutrition does not support muscle rebuilding. Low protein intake leads to rapid muscle loss in the residual limb, core, and opposite limb. Weak muscles mean poor balance, low endurance, and slow gait training once the prosthesis is introduced.
For prosthetic use, muscle strength is not optional. It decides how well a patient controls the device, how long they can wear it, and how confident they feel. Nutrition, especially protein, is the foundation of this strength.
Most early prosthetic failures are due to skin issues, not device issues. Fragile skin, delayed wound closure, repeated breakdown, and pressure sores are all linked strongly to poor nutrition. Protein, fluids, and basic micronutrients keep skin elastic and resistant to pressure.
When nutrition is poor, even a well-fitted socket becomes painful. This leads to reduced wear time, fear of the prosthesis, and repeated clinic visits. Optimizing nutrition early reduces these problems significantly.
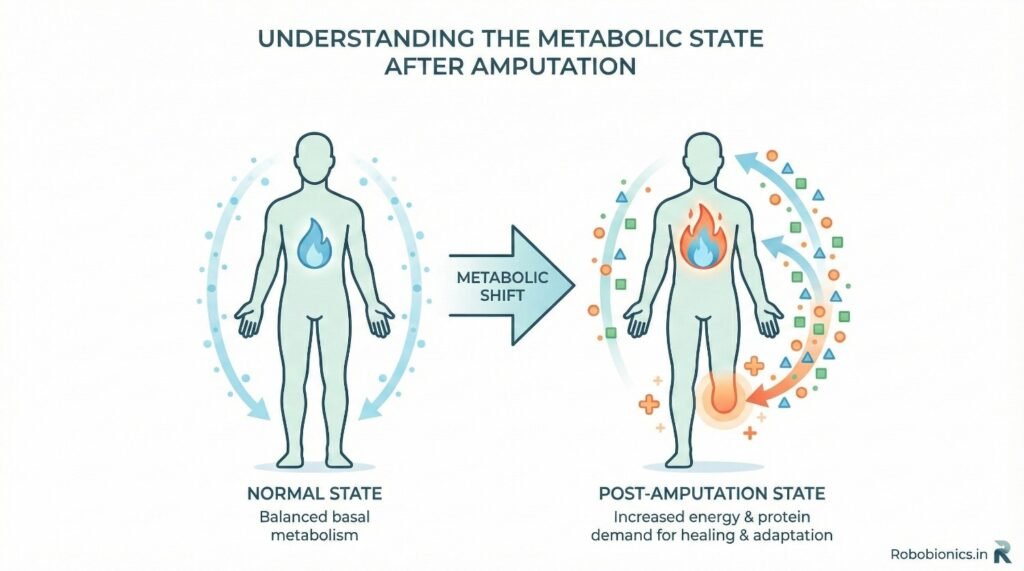
Amputation is a major physical stress. The body responds by increasing energy use, breaking down muscle, and prioritizing healing. This stress response increases calorie and protein needs, even if the patient is resting most of the day.
Many patients eat less during this time due to pain, low mood, or hospital routines. This mismatch between need and intake creates a hidden deficit that slows recovery.
Inflammation is part of healing, but it also increases nutrient use. Protein is used faster, vitamins are consumed quickly, and fluid balance becomes delicate. If intake does not match this increased demand, healing quality suffers.
For MDs, understanding this metabolic shift explains why “normal diet” is often not enough after amputation.
Older patients, diabetics, and vascular cases have lower reserves to begin with. Even short periods of low intake can push them into deficiency. These patients may not lose visible weight but still lose muscle and healing capacity.
Early nutrition screening is critical in this group.
Protein is needed to rebuild muscle, strengthen skin, support immunity, and heal wounds. Without enough protein, no amount of therapy or prosthetic training will work well. This is why protein targets should be discussed as seriously as medicines.
Many patients believe protein is only for bodybuilders. Simple education corrects this and improves compliance.
After amputation, protein needs are higher than normal. Most patients require significantly more protein per day than before surgery. The exact amount depends on body weight, wound status, and activity level, but the principle remains the same: intake must be intentional, not accidental.
MDs should give clear targets rather than vague advice. Patients follow numbers better than general statements.
Protein works best when spread across the day. One heavy meal does not compensate for a low-protein day. Regular intake supports steady healing and muscle repair.
Encouraging protein at each meal improves overall intake without overwhelming the patient.
Even with good protein intake, low calories force the body to burn protein for energy instead of healing. This leads to muscle loss and delayed wound repair. Patients who eat “light” thinking it helps recovery often slow it instead.
Clear explanation helps patients understand that food is medicine during this phase.
Some patients worry about weight gain before prosthetic fitting. While excessive weight gain is not ideal, aggressive calorie restriction is far worse. The priority before prosthesis is strength, healing, and endurance.
Weight can be managed later. Weakness delays prosthetic success much more than moderate weight gain.
Pain, medicines, and low mood reduce appetite. Smaller, frequent meals work better than large portions. Nutrient-dense foods help patients meet needs without feeling full.
MD guidance reassures patients that eating despite low hunger is part of treatment.
Poor hydration thickens blood flow and reduces nutrient delivery to healing tissues. Skin becomes dry and fragile, increasing risk of breakdown during socket use.
Simple hydration targets improve tissue tolerance significantly.
Some patients reduce fluid intake to control swelling. This often backfires. Proper hydration actually supports fluid balance and reduces edema when combined with compression and movement.
Clear explanation prevents this common mistake.
Hydration plans must be adjusted carefully in patients with heart or kidney disease. Coordination with treating physicians ensures safety while still supporting healing.
Individualization is key.
Iron, zinc, vitamin C, and vitamin D play major roles in healing and muscle function. Deficiency slows recovery even if calories and protein are adequate.
Basic screening and supplementation where needed can make a visible difference.
Whole foods provide a wide range of nutrients that work together. Supplements are helpful when intake is poor or deficiency is confirmed, but they should not replace proper meals.
Simple food-based advice improves long-term habits.
Diabetes, infections, and long hospital stays increase micronutrient loss. These patients often benefit from closer monitoring and targeted supplementation.
Early correction prevents long delays later.
Nutrition should support rehab, not fight it. Eating protein and some calories before or after therapy improves strength gains and reduces fatigue.
Patients who feel stronger participate better in training.
Skipping meals increases muscle breakdown and fatigue. Regular meals stabilize energy and mood, which improves rehab engagement.
Hospital routines should be adjusted where possible.
Before early socket trials or standing sessions, adequate nutrition improves tolerance. Patients with low energy or low protein often report more pain and fear.
Small changes in timing improve experience significantly.
For most amputees, protein needs increase clearly after surgery and stay high until prosthetic use becomes stable. This is not a short phase. Healing, muscle rebuilding, and skin strengthening continue for weeks or months. A general medical rule is that protein intake should be clearly higher than pre-surgery levels and maintained consistently, not just for a few days.
Patients should be told that protein is not a temporary supplement but a daily requirement during recovery. When this is explained clearly, compliance improves.
Younger patients with traumatic amputations often have higher muscle mass and higher activity goals. Their protein needs are higher because they aim to return to work, sports, or physically demanding roles. They also tend to start rehab earlier, which increases protein use.
These patients often underestimate their needs because they appear “healthy.” Clear targets prevent muscle loss and speed prosthetic control training.
These patients often need protein even more urgently, despite lower activity levels. Poor circulation and chronic disease slow healing, and protein supports tissue repair and immunity. Many of these patients eat less due to long illness, appetite loss, or food restrictions.
Medical guidance should focus on safe, adequate protein without worsening sugar control. This balance is achievable with planning and education.
Older patients lose muscle faster and rebuild it more slowly. Protein intake must be steady and spread across the day. Large single meals are less effective. Small, frequent protein portions work better and are easier to tolerate.
Explaining this simply to caregivers improves adherence.
Telling patients to “eat more protein” is not enough. They need to know what this looks like on a plate. Real food examples work better than nutrition charts. Patients understand eggs, milk, dal, curd, paneer, fish, and chicken far better than grams alone.
Clear daily examples help patients and families plan meals confidently.
Many Indian diets are high in carbohydrates and low in protein. This is not a problem in normal life, but it becomes a problem after amputation. Roti, rice, and potatoes fill the stomach but do not support healing alone.
Encouraging small protein additions to familiar meals is more effective than drastic diet changes. This approach respects culture and improves long-term compliance.
Vegetarian patients can meet protein needs with planning. Dairy, pulses, soy, and nuts play an important role. The key is variety and quantity. Single sources alone are often not enough.
MD reassurance reduces fear that vegetarian diets are inadequate.
Many patients intentionally reduce food intake after amputation due to fear of weight gain. This is one of the most damaging mistakes. Muscle loss and weak healing delay prosthetic use far more than mild weight gain.
Clear medical advice helps patients prioritize recovery over short-term weight concerns.
Protein powders and drinks can help, but they cannot replace meals completely. Patients who skip meals and rely only on supplements often miss calories and micronutrients.
Supplements should support, not replace, food.
Healing does not end when stitches are removed. Muscle rebuilding and skin adaptation continue into prosthetic training. Stopping nutrition focus too early leads to fatigue, pain, and poor prosthetic tolerance.
MD follow-up should reinforce continued nutrition support.
A well-nourished limb tolerates pressure better. Skin stays flexible, tissues adapt faster, and pain reduces over time. Poor nutrition leads to sensitivity, frequent redness, and fear of wearing the prosthesis.
This link should be explained clearly to patients to improve motivation.
Protein and fluids reduce friction injuries and speed recovery from minor skin issues. This prevents forced breaks from prosthetic use.
Consistent intake supports consistent wear time.
Nutrition affects fluid balance and muscle tone. Poor intake can cause limb volume changes, affecting socket fit and comfort. Stable nutrition supports stable fitting.
This reduces repeated adjustments and patient frustration.
Good nutrition does not mean poor sugar control. Balanced meals with adequate protein actually improve glucose stability. Skipping meals or eating only carbohydrates worsens fluctuations.
Clear guidance reduces fear around eating.
In patients with kidney disease, protein targets must be individualized. Coordination with nephrology is important. Even in these cases, completely low protein intake often harms healing.
Balanced plans protect both healing and kidney function.
Infections increase protein and calorie needs further. During these periods, nutrition must be actively supported to avoid rapid muscle loss.
Early nutrition support shortens recovery time.
Patients take nutrition seriously when doctors discuss it, not only dieticians. A few clear sentences from an MD often have more impact than long counseling sessions.
This influence should be used intentionally.
Basic screening for weight loss, appetite, and muscle loss identifies risk early. Simple documentation ensures continuity across teams.
Early action prevents delays.
Dieticians provide detailed plans, but MD alignment improves compliance. Involving caregivers ensures plans are followed at home.
Teamwork improves outcomes.
Prosthetic training requires concentration and effort. Poor nutrition leads to fatigue and frustration. Patients who eat well learn faster and retain skills better.
This improves confidence and reduces dropout.
Adequate calories and protein support longer wear time without excessive pain. This allows faster progression from short trials to daily use.
Nutrition becomes a hidden performance factor.
Well-nourished patients often report lower pain and better tolerance. Healing tissues respond better to stress when supported properly.
This improves overall experience.
When nutrition is framed as treatment, not advice, compliance improves. Patients understand that food supports recovery just like medicines.
Clear language builds seriousness.
Families often control food choices. Educating them prevents conflict and confusion. Simple instructions work best.
Support at home matters.
Good nutrition habits built before prosthesis often continue after fitting. This supports long-term comfort and health.
Early education has lasting value.
Nutrition works best when it is not treated as optional advice but as a routine clinical step. In many hospitals, food intake is discussed only when weight loss becomes obvious. By then, muscle loss and poor healing have already started. A structured nutrition protocol ensures that every amputee is assessed early, guided clearly, and followed up regularly. This reduces variation in care and improves prosthetic readiness across patient groups.
For MDs, standard protocols reduce guesswork. When nutrition targets are built into admission notes, discharge summaries, and rehab plans, patients receive consistent messages. This consistency alone improves adherence and reduces delays caused by preventable weakness or skin issues.
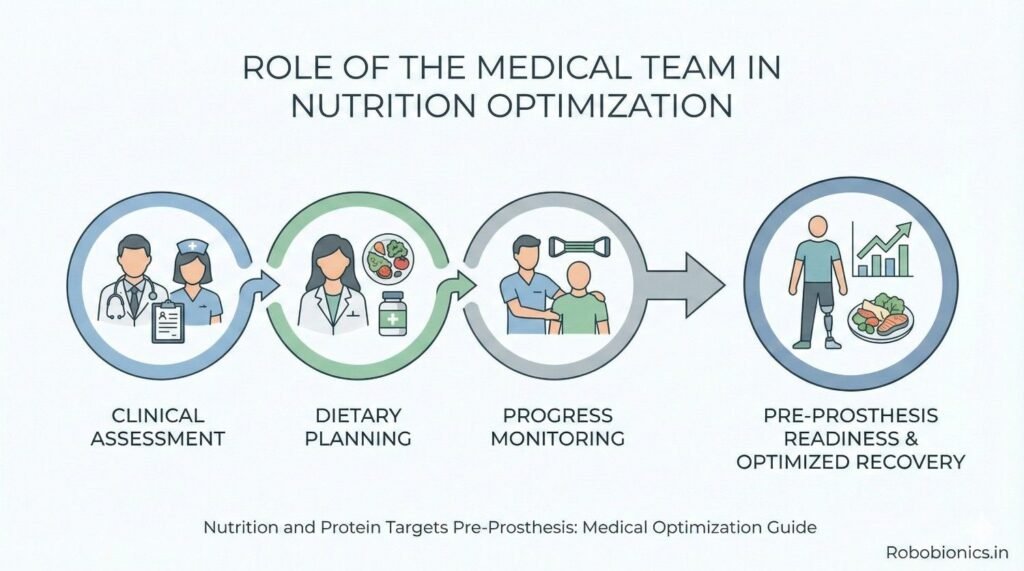
Nutrition screening does not need complex tools. Simple questions about recent weight loss, appetite, meal frequency, and fatigue identify most at-risk patients. Visual assessment of muscle wasting and skin quality adds valuable clinical insight. When these checks are done early, interventions can begin before delays appear.
Documenting these findings ensures that downstream teams understand nutritional risk and act early rather than react late.
Nutrition often fails when responsibility is unclear. Clear assignment of roles improves outcomes. MDs set targets and explain importance, dieticians refine plans, nurses reinforce intake, and therapists link nutrition to performance. When everyone reinforces the same message, patients take it seriously.
This shared ownership turns nutrition from advice into action.
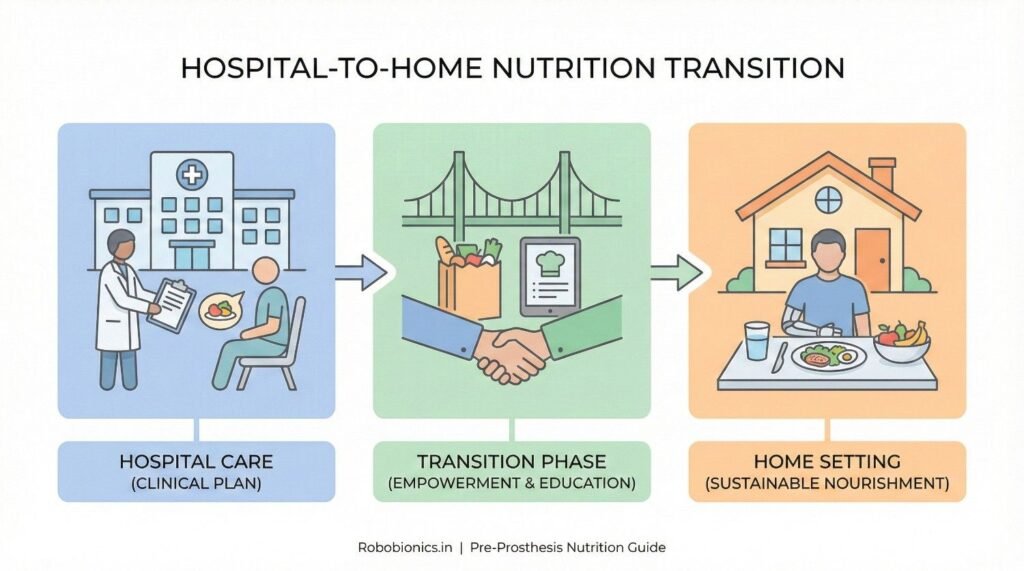
Many patients eat better in hospital than at home due to routine and supervision. Once discharged, intake often drops due to fatigue, cost concerns, or lack of guidance. A strong discharge nutrition plan prevents this drop. Clear written instructions, simple food examples, and realistic targets help patients maintain intake at home.
MDs who review nutrition plans during discharge reinforce its importance and improve compliance.
Patients return to different home environments. Some have strong family support, while others manage alone. Nutrition plans must adapt to these realities. Simple, easy-to-prepare foods work better than complex recipes. Affordable protein sources should be prioritized.
Practicality decides success more than ideal recommendations.
Early follow-up allows quick correction of problems. Appetite loss, digestive issues, or confusion about diet can be addressed before they affect healing. Telephonic or short outpatient reviews are often enough to maintain momentum.
Small check-ins prevent major setbacks.
Prosthetic fitting places new stress on skin and soft tissue. Well-nourished tissues adapt faster and resist injury. Patients who enter fitting with good protein stores and hydration experience less soreness and recover faster between sessions.
This improves confidence and reduces fear of the prosthesis.
Early prosthetic use requires mental focus and physical endurance. Nutrition supports both. Stable blood sugar, adequate calories, and sufficient protein reduce fatigue and frustration. Patients learn movements faster and retain skills better.
This speeds up the overall rehabilitation timeline.
Early prosthetic discomfort can discourage patients. Nutrition reduces pain sensitivity and improves recovery between sessions. Patients who feel physically stronger are more willing to continue despite mild discomfort.
This resilience is often the difference between success and abandonment.
Bilateral amputees face very high energy and protein demands. Mobility training is intensive, and muscle use is high. Nutrition deficits appear quickly and have severe effects. Early, aggressive nutrition support is essential to avoid rapid weakness and delayed prosthetic progress.
Clear targets and close monitoring are critical in this group.
Prolonged hospitalization increases muscle loss even with normal food intake. Bed rest accelerates weakness. Nutrition plans must account for this and often need to be more aggressive.
MD awareness prevents underestimation of needs.
Low mood reduces appetite and compliance. Nutrition suffers silently in these patients. Gentle encouragement, simple goals, and family involvement help maintain intake.
Addressing emotional health supports nutritional success.
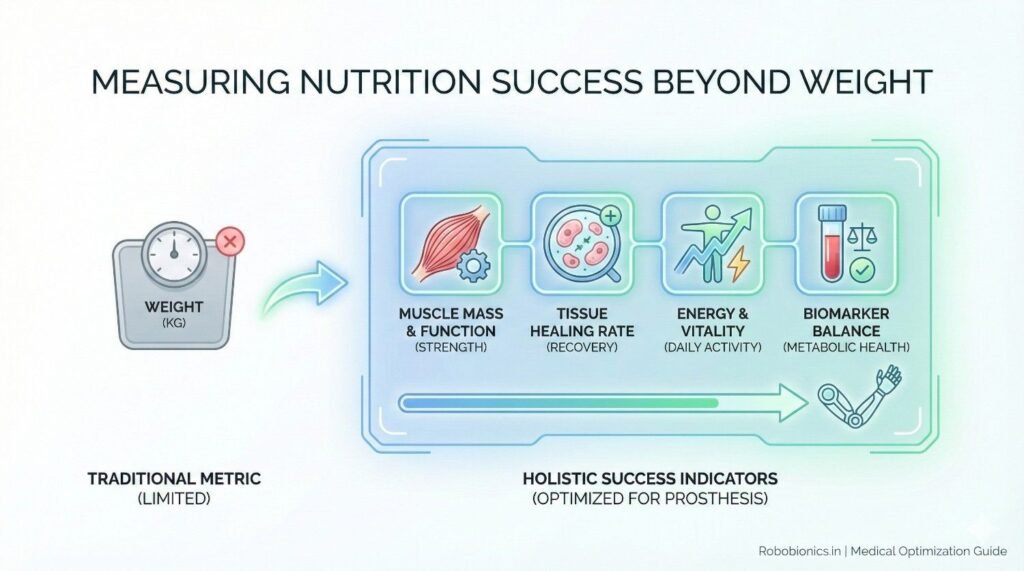
Weight alone does not reflect nutrition status. Muscle strength, endurance, wound quality, and skin tolerance provide better indicators. Patients may maintain weight while losing muscle and healing capacity.
MDs should track functional progress alongside nutrition.
Improving tolerance to compression, handling, and socket contact often signals good nutrition. Delayed tolerance may suggest underlying deficits even if wounds appear healed.
This clinical insight guides adjustments.
Patients who feel more energetic and less fatigued often have adequate intake. Fatigue without clear cause should prompt nutrition review.
Listening to patients provides valuable clues.
Overly complex nutrition advice confuses patients. Simple messages repeated consistently work best. Linking food choices to healing and independence improves motivation.
Clear communication drives behavior change.
Some patients fear eating due to medical conditions or misinformation. Clear reassurance reduces anxiety. When patients feel safe eating, intake improves naturally.
MD reassurance carries strong weight.
Patients who understand why nutrition matters take ownership of their recovery. This sense of control improves adherence and long-term outcomes.
Empowerment improves success.
Prosthetists see the impact of nutrition on skin and comfort directly. When they reinforce nutrition messages, patients connect cause and effect clearly.
This cross-team reinforcement strengthens compliance.
Prosthetic fitting issues often reflect nutrition problems. Feeding this information back to MDs allows early correction.
Collaboration improves efficiency.
When all teams emphasize nutrition as part of prosthetic success, patients hear a unified message. This reduces confusion and improves adherence.
Consistency builds trust.
Before prosthetic fitting, nutrition is a core medical intervention. It decides healing speed, muscle strength, skin health, and confidence. Treating it casually delays outcomes.
MDs should give it the same importance as medicines and therapy.
Protein intake supports everything the prosthesis depends on. Clear targets, practical guidance, and consistent follow-up ensure success.
Without protein, progress stalls.
Nutrition deficits are easier to prevent than correct. Early screening, education, and planning save weeks or months later.
Time invested early pays off.
Patients who are nutritionally optimized adapt faster, tolerate prostheses better, and regain independence sooner. This improves quality of life and reduces healthcare burden.
Medical teams play a central role in enabling this success.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body