
Post-Op Follow-Up Schedule That Prevents Prosthetic Delays (For Clinicians)
For many clinicians, the surgery is only the first step. What happens after the operation


Pain after amputation is one of the most confusing and emotionally difficult experiences for patients. Many people expect pain to come from the surgical area, yet they feel pain in a limb that no longer exists. Others experience burning, stabbing, or electric sensations that seem to come from deep inside the nerves. These experiences raise an important question for doctors and patients alike: does phantom pain or neuropathic pain affect prosthetic eligibility?
At Robobionics, we work closely with amputees who are eager to return to function but are held back by pain that feels unpredictable and frightening. Some worry that pain means they are not suitable for a prosthetic. Others rush into prosthetic use hoping it will make the pain disappear. Both assumptions can lead to disappointment if not guided properly.
This article explores phantom pain and neuropathic pain in the context of prosthetic eligibility. It explains what these pain types really are, how they behave over time, and how they interact with prosthetic fitting and use. The focus is not on fear, but on clarity. Pain does not automatically disqualify a patient, but it must be understood, respected, and managed carefully.
If you are a clinician, therapist, or amputee trying to make sense of pain after limb loss, this guide will help you make informed decisions. Prosthetic care works best when pain is addressed honestly and proactively, not ignored or rushed past.
Phantom pain is pain that feels like it is coming from the missing limb.
Patients may describe squeezing, burning, stabbing, or twisting sensations.
The pain feels real even though the limb is no longer there.
This pain comes from changes in the brain and spinal cord, not from the limb itself.
The brain still holds a map of the missing limb and continues to send signals.
This explains why the pain can feel vivid and specific.
Phantom pain is very common after amputation.
Experiencing it does not mean something has gone wrong.
It is a known response of the nervous system to limb loss.
Neuropathic pain comes from injured or irritated nerves.
After amputation, nerves are cut and must heal or adapt.
Sometimes this process leads to abnormal pain signals.
Patients often describe neuropathic pain as electric, sharp, or shooting.
It may occur at the residual limb or travel up the limb.
Touch or pressure can sometimes trigger it.
Neuropathic pain behaves differently from surgical pain.
It may persist long after wounds heal.
Understanding its pattern is important for prosthetic planning.
Phantom pain feels like it comes from the missing limb.
Neuropathic pain usually follows the path of damaged nerves.
Both can exist together in the same patient.
Phantom pain is driven more by the brain’s memory of the limb.
Neuropathic pain is driven by nerve damage and sensitivity.
Each responds differently to treatment.
For prosthetic decisions, the distinction matters.
Management strategies differ.
Eligibility depends on control, not just presence of pain.
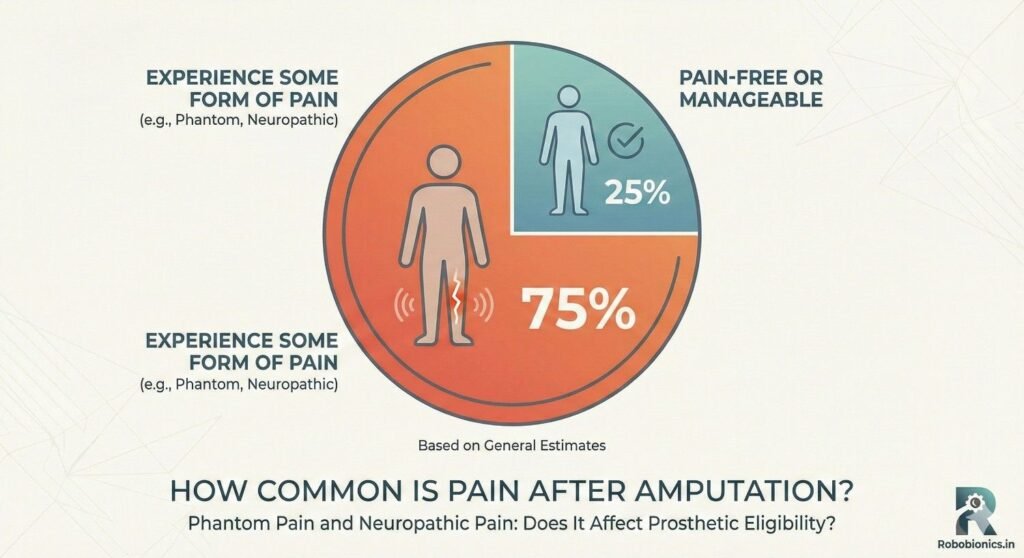
Most amputees experience phantom pain at some point.
For many, it appears early after surgery.
For others, it develops weeks or months later.
The intensity varies widely.
Some feel mild discomfort that fades over time.
Others experience severe episodes that interfere with daily life.
Importantly, phantom pain often changes.
It may reduce with time and activity.
This natural course influences prosthetic timing.
Neuropathic pain is also common after amputation.
It depends on nerve injury, surgical technique, and healing.
Certain conditions increase the risk.
Patients with diabetes or vascular disease may be more affected.
Poor nerve healing increases sensitivity.
Pain may fluctuate with fatigue or stress.
Neuropathic pain tends to persist if untreated.
Early recognition improves outcomes.
This is crucial before prosthetic fitting.
No two nervous systems respond the same way.
Genetics, prior pain experience, and mental state all play a role.
This explains wide variation in pain severity.
Emotional stress can amplify pain signals.
Poor sleep and anxiety worsen perception.
Pain is never purely physical.
Doctors must assess each patient individually.
Assumptions based on averages fail.
Personalized evaluation supports better decisions.
Having phantom or neuropathic pain does not automatically rule out prosthetic use.
Many successful prosthetic users continue to experience some pain.
What matters is how the pain behaves.
If pain is predictable and manageable, prosthetic use may still be safe.
If pain overwhelms attention or balance, caution is needed.
Eligibility depends on control, not diagnosis.
Patients should be reassured early.
Pain does not mean prosthetics are impossible.
Fear often worsens pain perception.
Pain affects focus and movement quality.
Severe pain can distract patients during walking or standing.
This increases fall risk.
Sudden pain spikes may cause hesitation or collapse.
This is especially dangerous in lower limb users.
Safety becomes the primary concern.
Doctors must assess whether pain interferes with attention.
Functional testing helps clarify this.
Safety always overrides urgency.
Pain intensity alone is not enough to judge eligibility.
Two patients with similar pain levels may function very differently.
Tolerance and coping skills matter.
Some patients learn to work around pain safely.
Others become guarded and fearful.
Observation during tasks reveals these differences.
Eligibility decisions must consider behavior, not just pain scores.
This avoids unfair exclusion.
Functional reality guides care.
A poorly fitting prosthetic can worsen neuropathic pain.
Excess pressure irritates sensitive nerves.
This leads to increased discomfort.
Good socket design can reduce pain triggers.
Even pressure distribution calms irritated tissue.
Comfort improves confidence.
Fit adjustments are often needed in painful cases.
This is expected, not failure.
Close follow-up is essential.
For some patients, prosthetic use reduces phantom pain.
Movement and sensory input help reorganize brain signals.
This can quiet phantom sensations.
Weight bearing and activity provide feedback to the nervous system.
This feedback helps recalibrate perception.
Not all patients experience this benefit.
Doctors should not promise pain relief.
Improvement is possible but unpredictable.
Honest discussion prevents false hope.
In some cases, early prosthetic use aggravates pain.
This happens when nerves are highly sensitive.
Excess stimulation overwhelms adaptation.
Patients may report increased burning or sharp pain.
This signals the need to slow down.
Pushing through pain is rarely helpful.
Gradual exposure is safer.
Short wear times allow adaptation.
Listening to pain signals protects outcomes.
Doctors must explore pain carefully.
Onset, quality, triggers, and duration matter.
Vague questions miss important clues.
Patients should describe pain in their own words.
Patterns reveal underlying mechanisms.
This guides management decisions.
Pain diaries can be helpful.
They show fluctuation over time.
This supports timing decisions.
Clinical examination helps separate phantom and neuropathic pain.
Tapping nerves may reproduce neuropathic pain.
Phantom pain often lacks local triggers.
Understanding the dominant pain type matters.
Treatment approaches differ.
Eligibility planning depends on this clarity.
Doctors should avoid labeling all pain the same.
Precision improves care.
This reduces frustration.
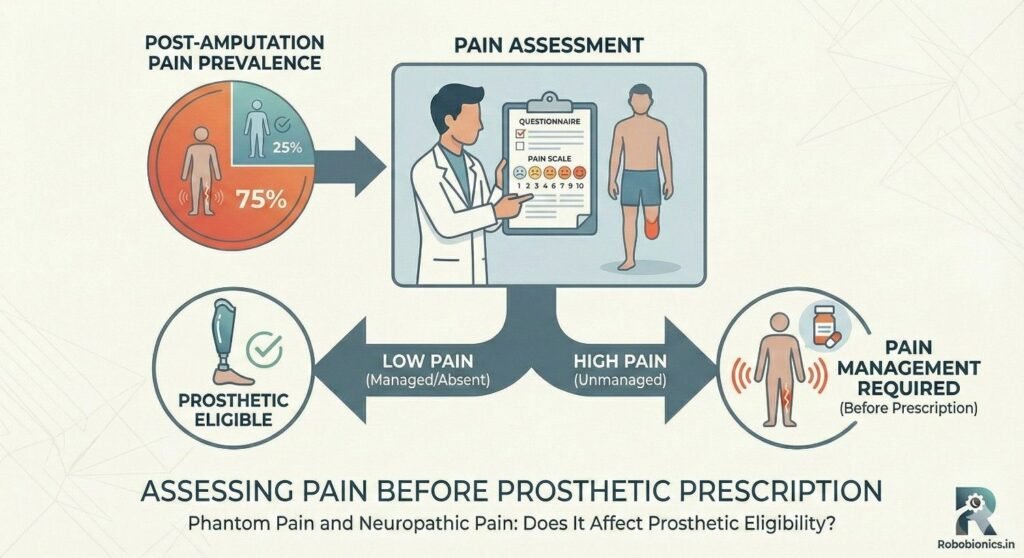
Pain should be assessed during movement.
Static pain at rest is less relevant than pain during activity.
Functional impact matters most.
Doctors should observe gait, transfers, and balance.
Pain-related hesitation is informative.
This reveals real-world risk.
Eligibility decisions should be based on observed performance.
This avoids overreliance on self-report.
Function guides safety.
Pain does not need to disappear before prosthetic fitting.
It does need to be reasonably stable.
Uncontrolled pain undermines training.
Stabilization means predictable patterns.
Patients can anticipate and manage symptoms.
This supports safe learning.
Doctors should aim for control, not perfection.
Waiting for zero pain may delay care unnecessarily.
Balance is key.
Medications may help manage neuropathic pain.
They aim to calm nerve signaling.
Response varies between patients.
Pain specialists can support complex cases.
Multimodal treatment often works best.
Medication alone is rarely enough.
Doctors should review side effects carefully.
Sedation affects prosthetic safety.
Monitoring is essential.
Physical therapy, mirror therapy, and desensitization can help.
These approaches retrain the nervous system.
They are especially useful for phantom pain.
Relaxation and breathing techniques reduce pain amplification.
Stress worsens symptoms.
Simple strategies improve tolerance.
Integrating these methods improves readiness.
Pain becomes less dominant.
This supports prosthetic success.
Pain often creates fear of movement.
Patients may avoid loading the limb.
This limits progress.
Avoidance increases stiffness and sensitivity.
Pain then worsens.
This cycle must be addressed.
Education helps break this pattern.
Safe movement reduces fear.
Confidence improves outcomes.
Stress amplifies pain signals.
Anxiety increases nerve sensitivity.
Mood directly affects pain experience.
Patients coping with limb loss face emotional strain.
This interacts with pain.
Support matters.
Psychological support should be offered early.
Addressing emotions improves physical outcomes.
Holistic care works best.
Some patients interpret pain as a sign of harm.
They may believe movement is dangerous.
This belief limits function.
Doctors should identify catastrophic thinking.
Reframing pain as manageable helps.
Education changes behavior.
Eligibility improves when fear is reduced.
Pain feels less threatening.
Confidence supports safe use.
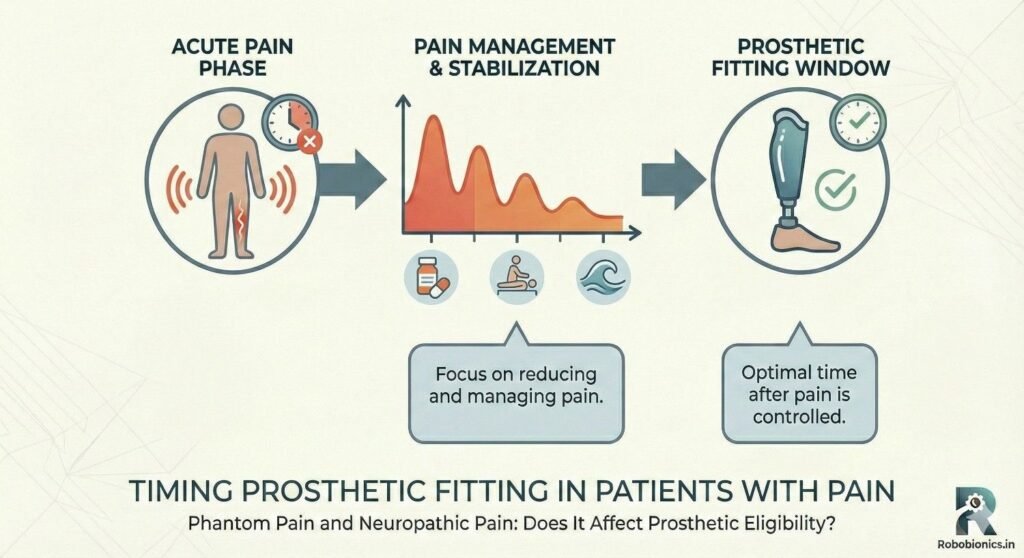
Early fitting may help some patients adapt.
It provides sensory input quickly.
This may reduce phantom pain.
For others, early fitting overwhelms sensitive nerves.
Delayed fitting allows stabilization.
Timing must be individualized.
Doctors should avoid rigid timelines.
Pain behavior guides decisions.
Flexibility improves safety.
Pain-sensitive patients benefit from gradual exposure.
Short wear times reduce overload.
The nervous system adapts slowly.
Incremental increases build tolerance.
Patients gain confidence.
Setbacks are minimized.
Doctors should set clear expectations.
Slow progress is still progress.
Patience pays off.
Pain should be monitored continuously.
Worsening trends signal need for adjustment.
Ignoring pain delays recovery.
Doctors should encourage honest reporting.
Patients should not hide pain to please clinicians.
Open communication protects safety.
Training plans should remain flexible.
Adaptation requires feedback.
Responsive care improves outcomes.
Phantom and neuropathic pain rarely stay the same over time, especially once a patient begins using a prosthetic in daily life.
In many cases, regular movement, weight bearing, and sensory input help calm the nervous system and reduce the frequency or intensity of phantom pain episodes.
The brain slowly updates its internal map, which can make pain feel less sharp or less intrusive during activity.
However, this improvement is not automatic and does not happen for everyone.
Some patients notice that pain reduces during activity but returns during rest, while others experience flare-ups when they overdo training.
Understanding this evolving pattern helps doctors guide patients without creating unrealistic expectations.
For a smaller group of patients, pain remains persistent and dominant despite time and treatment.
In these cases, pain may drain attention, disrupt sleep, and reduce tolerance for training, which directly affects prosthetic use.
This does not mean prosthetics are impossible, but it does mean goals may need adjustment.
Chronic pain often shifts the focus from performance to comfort and safety.
Shorter wear times, simpler prosthetic designs, or part-time use may be more appropriate.
Recognizing this early prevents frustration and emotional burnout.
It is important to separate constant pain from high sensitivity to stimulation.
Some patients have low pain thresholds but recover quickly after stimulation, while others experience prolonged pain after minor triggers.
This difference matters greatly for prosthetic planning.
Patients with high sensitivity may still use a prosthetic safely if exposure is gradual and well controlled.
Those with prolonged pain responses may need longer stabilization before increasing use.
Observation over time provides clearer guidance than one-time assessments.
Pain becomes a prosthetic eligibility concern when it interferes with balance or awareness during movement.
If a patient freezes, hesitates, or suddenly shifts weight because of sharp pain, the risk of falling increases significantly.
This is especially relevant for lower limb prosthetic users.
Doctors should pay close attention to how patients respond to pain during standing and walking tasks.
Momentary distraction may be manageable, but repeated disruption signals the need for caution.
Safety must guide eligibility decisions in these situations.
Pain that appears suddenly without clear triggers is harder to manage during prosthetic use.
Unpredictable spikes make it difficult for patients to plan activity or protect themselves.
This uncertainty increases fear and hesitation.
When pain behavior is erratic, doctors may recommend delaying fitting or limiting use until patterns become clearer.
Stabilization through medical or therapeutic intervention often improves predictability.
Predictable pain is easier to manage than severe but consistent pain.
Pain rarely exists in isolation, and its impact is amplified when combined with anxiety, depression, or reduced concentration.
Patients who become overwhelmed by pain may struggle to follow safety instructions or respond quickly to balance challenges.
This combination increases overall risk.
Doctors should assess pain alongside emotional and cognitive factors.
Eligibility decisions must reflect the full picture, not pain intensity alone.
Integrated assessment supports safer outcomes.
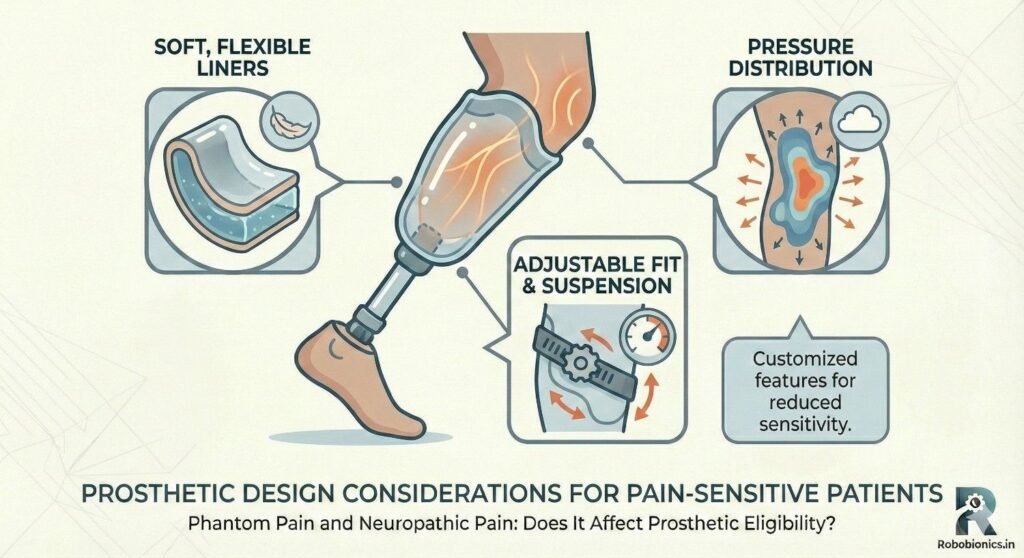
Socket comfort is one of the most important factors for patients with neuropathic pain.
Uneven pressure, sharp edges, or excessive compression can irritate sensitive nerves and worsen symptoms.
Even small fit issues may feel severe to these patients.
Careful socket design that distributes pressure evenly can significantly reduce pain triggers.
Frequent early adjustments are often necessary and should be expected.
Comfort is not a luxury but a requirement for pain-sensitive users.
Shock and vibration travel through the prosthetic into the residual limb and nervous system.
For patients with neuropathic pain, this input can aggravate symptoms and reduce tolerance.
Component choice plays a major role in managing this issue.
Prosthetic systems that absorb shock and smooth movement reduce nerve irritation.
Softer foot response or controlled movement patterns often feel safer and more comfortable.
Design decisions should prioritize nerve comfort as much as mechanical function.
Highly dynamic or aggressive prosthetic designs may demand rapid responses and higher loads.
For pain-sensitive patients, this can overwhelm adaptation and worsen symptoms.
A more forgiving design often supports better long-term use.
Doctors and prosthetists should resist the urge to push advanced technology too early.
Building tolerance first allows future progression if appropriate.
A staged approach protects both physical and emotional well-being.
Training with pain requires a careful balance between encouragement and respect for limits.
Patients should never feel pressured to ignore pain signals, as this erodes trust and safety.
Instead, pain should be acknowledged as part of the learning process.
Doctors and therapists should frame training as exploration rather than performance.
This reduces fear and allows patients to communicate honestly about discomfort.
A supportive tone improves engagement and outcomes.
The nervous system adapts best to gradual, predictable exposure.
Short, controlled prosthetic use allows the brain and nerves to adjust without overload.
This approach is especially important for neuropathic pain.
Incremental increases in wear time and activity help build tolerance.
Patients often find that pain becomes less threatening as confidence grows.
Consistency matters more than intensity during this phase.
Not all discomfort signals harm, but not all pain should be ignored.
Patients need help learning the difference between adaptation discomfort and warning pain.
This skill improves safety and confidence.
Doctors should explain signs that require stopping, such as sharp, escalating pain or loss of control.
Clear guidance reduces fear and confusion.
Education empowers patients to self-manage responsibly.
Pain specialists can provide valuable support when phantom or neuropathic pain is severe or persistent.
They offer expertise in medication management, nerve treatments, and coping strategies.
Early involvement often improves outcomes.
Referral does not mean prosthetic care must stop.
In many cases, pain management and prosthetic planning proceed together.
Collaboration strengthens decision-making.
Pain treatments may affect alertness, balance, or energy levels.
Doctors must consider these effects when planning prosthetic training.
Timing sessions to avoid peak side effects improves safety.
Close communication between teams ensures that adjustments are coordinated.
This prevents conflicting advice and confusion.
Unified care builds patient trust.
Pain response during treatment provides useful information about readiness.
Improvement in control or predictability often signals readiness to progress.
Worsening trends suggest the need to slow down.
Doctors should view pain response as feedback rather than a verdict.
This flexible approach keeps options open.
Patients feel supported rather than judged.
Many patients believe prosthetic fitting should wait until pain disappears completely.
In reality, waiting for zero pain is often unrealistic and unnecessary.
What matters is stability and manageability.
Doctors should explain that some pain can coexist with safe prosthetic use.
Clear education reduces fear and delay.
Balanced messaging improves readiness.
Some patients fear that prosthetic use will intensify phantom pain.
While this can happen temporarily, many experience no worsening or even improvement.
Responses vary widely.
Honest discussion about variability is essential.
Doctors should avoid absolute statements.
Realistic expectations reduce anxiety.
Severe pain does not automatically exclude prosthetic use.
It signals the need for careful planning and support.
Many patients with significant pain still achieve meaningful function.
Doctors should emphasize possibility rather than limitation.
Adaptive strategies expand options.
Hope grounded in realism supports resilience.

Eligibility discussions should focus on safety and long-term success rather than denial.
Patients need to understand that decisions are made to protect them, not restrict them.
Language matters greatly in these conversations.
Doctors should explain how pain affects attention, balance, and learning.
Connecting decisions to everyday safety makes them easier to accept.
Transparency builds trust.
Patients should be active participants in timing decisions.
Their experience of pain provides valuable insight.
Shared decision-making improves commitment.
Doctors should invite questions and concerns openly.
This reduces misunderstanding and fear.
Partnership strengthens outcomes.
Pain patterns change over time, and eligibility decisions should be revisited.
What is unsafe today may be manageable later.
Regular reassessment keeps care responsive.
Doctors should reassure patients that delay is not permanent.
Progress remains possible.
Flexibility supports hope and engagement.
Phantom pain and neuropathic pain should never be viewed in isolation when deciding prosthetic eligibility.
They are one part of a larger readiness picture that also includes strength, balance, endurance, cognition, and emotional resilience.
When pain is considered alongside these factors, decisions become clearer and fairer.
Doctors should avoid binary thinking where pain means either full approval or complete rejection.
Most patients fall somewhere in between and need tailored planning.
This nuanced view leads to safer and more successful outcomes.
Eligibility is not a single moment but a pathway that evolves over time.
Some patients may be ready for partial prosthetic use, limited wear time, or specific environments only.
Others may need a period of pain stabilization before any fitting begins.
By creating individualized pathways, doctors allow patients to move forward without being overwhelmed.
Progress becomes structured and predictable.
This approach reduces fear and improves cooperation.
Many patients feel urgency to “move on” after amputation and see prosthetics as the next milestone.
While this motivation is understandable, the nervous system often needs more time to adapt.
Rushing this process can worsen pain and delay long-term success.
Doctors must balance emotional urgency with biological readiness.
Clear explanation helps patients understand why timing matters.
Patience becomes easier when the purpose is clear.
Prosthetists play a key role in identifying how pain interacts with prosthetic contact and load.
Early involvement allows potential fit issues to be anticipated before they become problems.
This proactive approach saves time and reduces discomfort.
Observing how the residual limb reacts to gentle pressure provides valuable insight.
Sensitivity patterns guide socket design decisions.
This collaboration improves readiness planning.
For patients with neuropathic pain, prosthetic adjustment is not a one-time event.
Fit and comfort may change as pain patterns evolve.
Frequent early follow-ups should be expected and normalized.
Doctors should prepare patients for this reality.
Understanding that adjustment is part of the process reduces frustration.
Flexibility supports long-term use.
Clear communication between doctors and prosthetists is essential in pain-sensitive cases.
Sharing pain history, triggers, and response patterns improves design decisions.
This coordination prevents conflicting advice.
When teams work together, patients feel supported rather than confused.
Unified messaging builds trust.
Collaborative care improves outcomes.
Success does not always mean full-day prosthetic use or high activity levels.
For some patients, success means safe transfers, short walks, or specific functional tasks.
Pain-aware goals protect quality of life.
Doctors should help patients redefine success in realistic terms.
This reduces disappointment and pressure.
Meaningful function matters more than comparison.
Pain often limits how much prosthetic use can be sustained.
Pushing for maximal use may backfire.
Sustainable use supports independence without worsening symptoms.
Doctors should encourage pacing strategies.
Rest is part of effective use, not failure.
This mindset supports long-term engagement.
Pain levels may change months or years after fitting.
New triggers, health changes, or stress can alter tolerance.
Regular monitoring is essential.
Doctors should ask about pain trends during follow-up.
Early adjustment prevents decline.
Ongoing care protects outcomes.
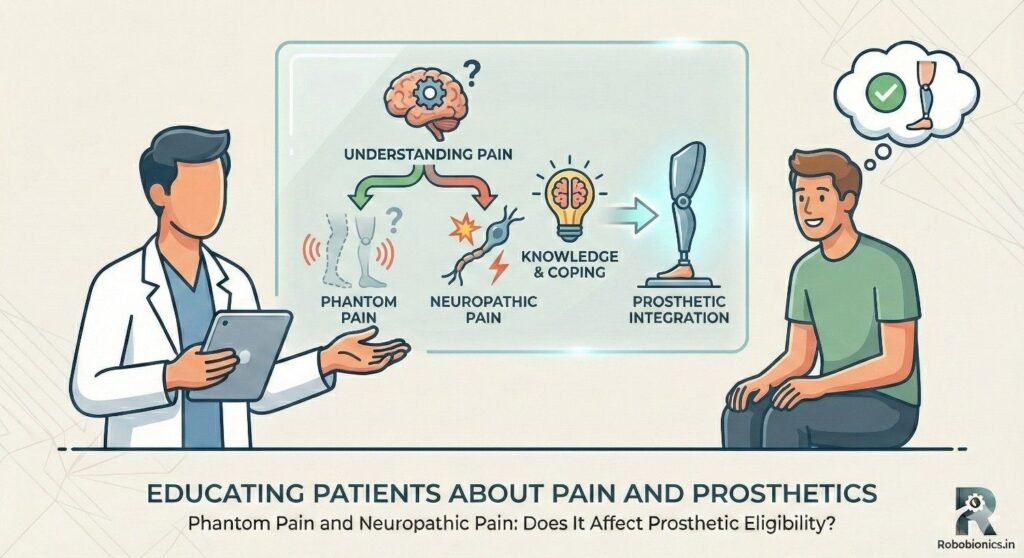
Patients benefit from honest, balanced information about pain and prosthetic use.
They should understand that pain may improve, worsen, or fluctuate.
Uncertainty should be acknowledged openly.
When expectations are realistic, patients cope better with setbacks.
Trust grows through honesty.
Education reduces fear-driven decisions.
Patients should be taught to observe their own pain patterns.
Recognizing triggers and early warning signs improves safety.
Self-awareness supports independence.
Doctors should encourage open reporting without judgment.
Patients should not feel they are “complaining.”
Pain information guides better care.
Education should empower patients to make informed choices.
Understanding pain helps patients feel in control rather than helpless.
Empowerment improves resilience.
When patients feel respected, they engage more fully.
Shared responsibility improves outcomes.
Knowledge becomes a tool, not a barrier.
Phantom pain and neuropathic pain are common after amputation, but they do not automatically determine prosthetic eligibility.
What matters is how pain behaves, how predictable it is, and how it affects safety, attention, and movement.
When pain is understood rather than feared, better decisions follow.
At Robobionics, we have seen that many patients with ongoing pain still achieve meaningful prosthetic use when care is thoughtful and paced correctly.
Pain management, prosthetic planning, and patient education must move together, not in isolation.
This integrated approach protects both physical function and emotional well-being.
Prosthetic eligibility is not about waiting for pain to vanish.
It is about ensuring pain is respected, managed, and integrated into care decisions.
When handled with clarity and compassion, pain becomes something to work with, not something that stops progress.
For many clinicians, the surgery is only the first step. What happens after the operation

For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body