
Trauma Amputees: ICU-to-Prosthesis Optimization Pathways for Doctors
For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much


For many clinicians, the surgery is only the first step. What happens after the operation often decides how soon a person can return to daily life with a prosthesis—or how long they remain stuck in delays, doubt, and discomfort.
Post-op follow-up is not just a routine task. It is the bridge between healing and function. When this phase is rushed, missed, or poorly planned, prosthetic fitting gets delayed. When it is done with care, structure, and clear timing, outcomes improve fast. Patients heal better. Clinics work smoother. Prosthetic teams can plan with confidence.
This article is written for clinicians who want fewer delays, fewer frustrated patients, and better long-term results. It is not theory-heavy. It is based on what actually works in real clinics, with real patients, and real constraints—especially in the Indian healthcare setting.
We will walk through a clear, practical post-op follow-up schedule that helps prevent common prosthetic delays. The focus is on timing, communication, wound readiness, and simple checks that make a big difference. No complex terms. No fluff. Just a system you can use and adapt.
When follow-up is done right, everyone wins.
In many cases, the delay does not come from the prosthetic side. It starts much earlier, during the healing phase. When follow-ups are irregular or unclear, the limb may heal slower than expected. Swelling, skin issues, or pain then push prosthetic timelines further away.
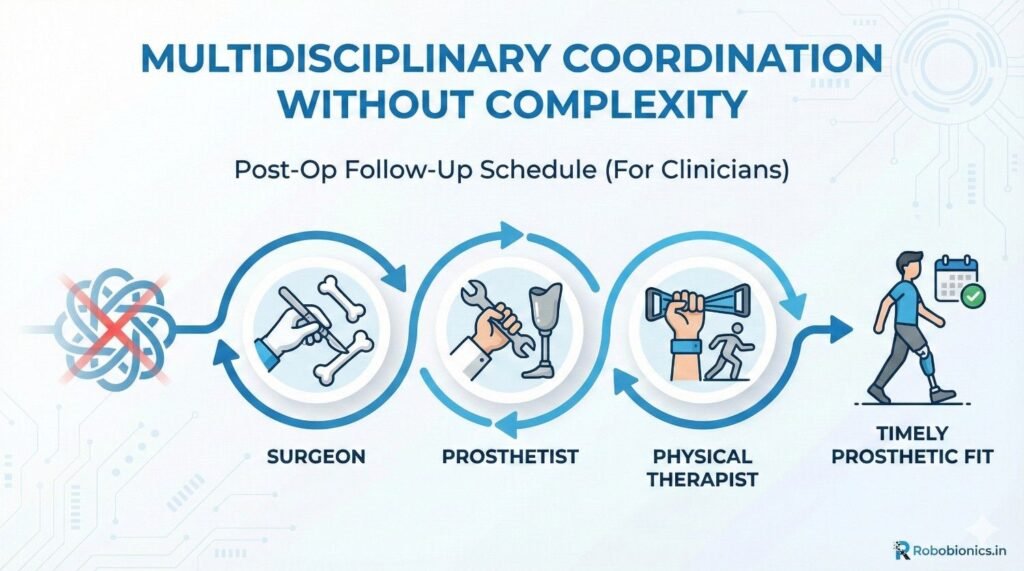
This gap often grows because no one owns the full journey. Surgeons focus on healing. Prosthetists focus on fitting. If the follow-up plan does not connect both, the patient stays in between with no clear next step.
A common issue is missed appointments. Patients may not understand why follow-up visits matter once the surgery feels “done.” Without clear guidance, they skip visits until a problem becomes visible or painful.
At the same time, clinics may not have a fixed follow-up flow. One patient is reviewed weekly, another after a month. This lack of structure makes it hard to plan prosthetic referrals on time.
What starts as a one-week delay often turns into months. Swelling that could have been managed early becomes chronic. Scars that needed early care become stiff and painful. Muscle strength drops because therapy started late.
Each small miss adds up. By the time prosthetic fitting is discussed, the limb is not ready. The patient feels frustrated, and the clinical team feels pressured.
The prevention of delay starts before discharge. Patients should know that surgery is only one part of recovery. Follow-up visits are not optional; they are part of treatment.
When clinicians explain this clearly, patients take follow-ups seriously. Simple words work best. Telling a patient that “these visits help you get your artificial limb faster” often makes the point clear.
Clinicians play a key role in linking surgeons, therapists, and prosthetists. Even a short update shared at the right time can save weeks of waiting.
When the treating clinician signals that healing is on track, prosthetic teams can prepare early. This overlap shortens the total recovery time.
Follow-ups are not just for checking wounds. They are checkpoints for future steps. Each visit should answer one simple question: “What is the next action needed to move toward prosthetic fitting?”
When follow-ups are used this way, delays become visible early and can be corrected quickly.
An effective schedule is based on fixed time points, not guesswork. Instead of saying “come back if there is a problem,” set clear dates.
Fixed schedules reduce confusion. They also help clinics plan staff time and prosthetic referrals more accurately.
Each follow-up visit should have one or two clear goals. Too many checks confuse both patient and clinician.
For example, one visit may focus only on wound healing. Another may focus on swelling and limb shape. Clear goals make visits faster and more useful.
Follow-ups should slowly shift focus from healing to readiness. Even when the limb is not ready, early signs can be tracked.
This approach allows prosthetic teams to be alerted early, even if fitting will happen later.
The first week after surgery is about protection. The wound must stay clean, dry, and safe from pressure.
Pain control is also key. When pain is managed well, patients move more. Movement improves blood flow and supports healing.
This is the best time to explain the recovery path. Patients and caregivers are attentive and want guidance.
Simple instructions work best. Explain what is normal, what is not, and when to call the clinic. Clear guidance reduces panic and unnecessary delays.
Before the patient leaves, the next visit should already be scheduled. A fixed date gives structure and reduces dropouts.
This visit should be explained as essential, not optional. Linking it to faster prosthetic use increases compliance.
At this stage, the focus is on how the wound is closing. Any open areas, redness, or discharge must be addressed early.
Skin health matters because prosthetic sockets depend on it. Poor skin now leads to poor fit later.
Swelling is expected, but it should reduce steadily. If swelling stays high, early steps like compression can be introduced.
Tracking limb shape early helps predict when prosthetic casting can begin. Even small notes in records help later planning.
Patients often feel better by this stage and may assume they are “almost done.” This is a key time to reinforce the next steps.
Clear words like “the next few weeks decide how well your prosthesis will fit” keep patients engaged.
By now, gentle movement should increase. This helps muscles stay active and prevents stiffness.
Clinicians should guide patients on safe movement, not just rest. Fear of movement can slow readiness for prosthetics.
Scars begin to mature during this phase. If scars become tight or painful, early care can prevent long-term problems.
Ignoring scar issues now often leads to socket pain later, which delays prosthetic use even after fitting.
This is a good time to introduce prosthetic planning, even if fitting is weeks away. Early discussion reduces fear and builds trust.
When patients know what is coming next, they are more patient and cooperative.
The limb should tolerate light pressure by now. Sensitivity checks help predict how well a socket will be accepted.
If sensitivity is high, early desensitization can be started. This saves time later.
This phase benefits most from team communication. A short update to the prosthetist helps them plan resources and timelines.
Even if casting is not immediate, early coordination reduces waiting lists and scheduling gaps.
Patients often expect immediate fitting once healing looks complete. Clinicians should explain remaining steps clearly.
Honest timelines build trust and prevent frustration when fitting does not happen overnight.
Many clinicians hesitate to refer patients to a prosthetist too early. There is a fear that the limb is not ready and the visit will be wasted. In reality, early referral is about planning, not fitting.
An early referral allows the prosthetic team to study the case, understand limb condition, and prepare for future steps. This reduces idle time later, when the limb is finally ready but no appointment is available.
A referral works best when it carries simple, clear details. The date of surgery, healing progress, current swelling status, and any skin concerns are often enough.
Long notes are not needed. What matters is clarity. When prosthetists receive useful information early, they can guide the next steps without delay.
Clinics that align follow-up visits with likely prosthetic milestones perform better. When a clinician knows that casting may happen in two weeks, follow-ups become more focused.
This alignment prevents the common problem of “healed but waiting,” where the patient is ready but the system is not.
Swelling is normal, but when it stays high for weeks, it becomes a problem. Many delays happen because swelling was observed but not acted upon early.
Simple steps taken at the right time often prevent months of waiting later. Clinicians who treat swelling as a priority see faster prosthetic readiness.
Even small skin issues can stop prosthetic fitting. Redness, fragile skin, or pain with touch are warning signs.
These issues rarely fix themselves. Early care during follow-ups avoids long pauses later when fitting must be stopped completely.
Muscle weakness and joint stiffness are silent delay factors. They may not seem urgent during healing, but they affect prosthetic use deeply.
Follow-ups that include basic movement checks catch these problems early and allow timely therapy support.
Busy clinics often struggle with documentation. The solution is not longer notes, but clearer ones.
Short updates that track progress over time help everyone involved. They allow patterns to be seen and decisions to be made faster.
Dates matter. So do trends. Is swelling reducing or stable? Is pain improving or unchanged? These small details guide prosthetic decisions.
When notes answer these questions clearly, back-and-forth communication reduces greatly.
Documentation helps only when shared. Clinicians should ensure that relevant updates reach therapists and prosthetists at the right time.
This does not require complex systems. Even simple shared records or scheduled updates can make a big difference.
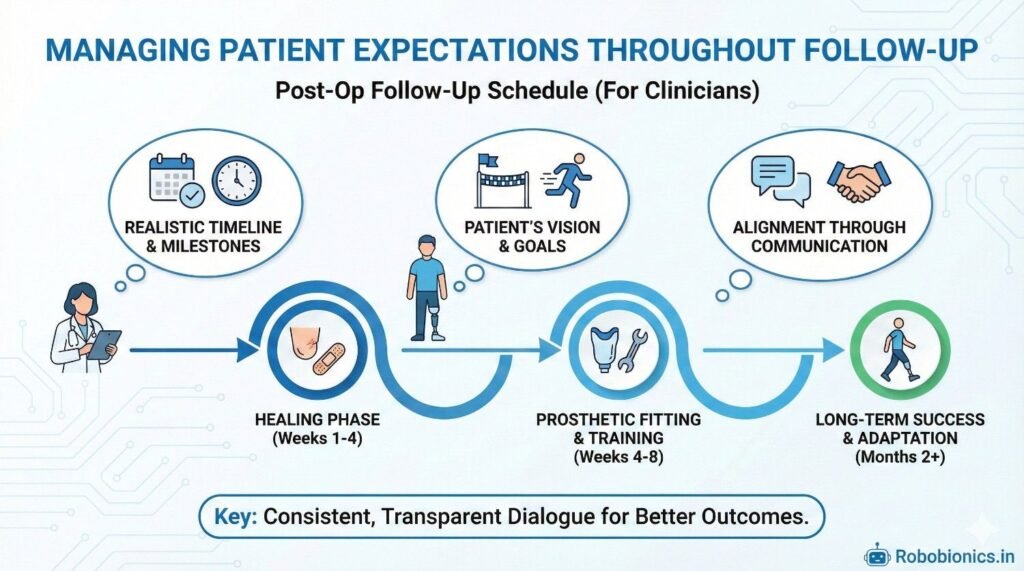
Patients often feel delays more strongly than clinicians expect. For them, every extra week feels like lost independence.
Clear communication during follow-ups helps patients understand why each step matters and why waiting is sometimes needed.
Saying “soon” or “in some time” increases anxiety. Giving rough timelines, even with flexibility, builds trust.
When patients know what to expect next, they are more patient and more engaged in their care.
Follow-ups are emotional moments. Patients look to clinicians not just for care, but for reassurance.
Balancing honesty with encouragement helps patients stay motivated without feeling misled.
Rehabilitation is often seen as optional in early healing. In reality, it is essential for prosthetic success.
Early therapy maintains muscle activity and joint range, which directly affects prosthetic control later.
Therapy works best when it prepares the patient for a prosthesis, not just general movement.
Clinicians who align therapy goals with future prosthetic use see smoother transitions into fitting and training.
Follow-up visits should include brief checks on therapy progress. This ensures that gaps are noticed early.
When therapy stalls, prosthetic readiness stalls too. Early correction saves time.
A defined follow-up flow reduces dependence on memory and individual judgment. It creates consistency across patients and staff.
When everyone knows what happens at each stage, delays reduce naturally.
A good schedule is firm but adaptable. It allows adjustments for individual healing while keeping the overall timeline intact.
This balance is key to preventing both rushing and unnecessary waiting.
A clear follow-up flow helps explain the process to patients and families. It sets expectations and reduces repeated questions.
When patients understand the plan, they are more likely to follow it.
Many follow-ups happen only when a problem appears. Advanced follow-up planning shifts this approach. Instead of reacting to issues, clinicians anticipate them.
When likely challenges are planned for in advance, solutions are ready before delays occur. This creates a smoother and faster path to prosthetic fitting.
Rather than focusing only on dates, milestone-based reviews focus on readiness markers. These include wound stability, swelling control, and limb tolerance.
When milestones guide follow-ups, decisions become clearer. Clinicians know exactly when to move forward and when to pause briefly for correction.
Not all patients need the same follow-up frequency. Some heal smoothly, while others face higher risks.
Patients with diabetes, vascular issues, or previous infections benefit from closer follow-up. Adjusting frequency early prevents late-stage setbacks.
Most clinicians agree teamwork is important, yet it often breaks down. The reason is not lack of intent, but lack of structure.
Without clear roles and timing, updates get missed. Patients then move slower through the system.
Every patient needs one clear clinical lead. This person tracks progress and ensures handovers happen on time.
When leadership is defined, communication improves. Decisions are made faster, and responsibility is clear.
Long meetings are not required. Short, regular updates work better.
A brief message at the right time often prevents weeks of delay later. Consistency matters more than detail.
Before prosthetic steps begin, the wound must meet basic readiness criteria. It should be closed, stable, and free from active infection.
Checking this early avoids failed casting attempts and repeated visits.
A limb that is still changing rapidly is not ready for fitting. Volume checks during follow-ups help predict stability.
When volume trends are tracked, prosthetic teams can plan casting at the right moment.
Basic muscle activation and joint movement are needed before prosthetic training.
Follow-ups that include simple movement checks prevent late surprises during fitting sessions.
Missed visits are rarely due to lack of care. Travel issues, cost concerns, and work pressures often play a role.
Clinicians who understand these reasons can adjust schedules and reduce dropouts.
Simple reminders improve attendance greatly. Clear instructions on why the visit matters also help.
Patients are more likely to return when they see direct benefit.
Flexibility does not mean no rules. It means offering alternate dates while keeping the follow-up goal intact.
This balance helps patients stay engaged without breaking the care flow.
Even with the best planning, some delays happen. Healing is not always predictable.
What matters is how quickly the delay is identified and addressed.
When delays occur, the follow-up plan should be reset openly. Patients should know what has changed and why.
Clear resets prevent confusion and loss of trust.
Delays affect morale. Follow-ups during waiting periods should include encouragement and guidance.
Keeping patients engaged emotionally helps maintain long-term success.
Physical readiness alone is not enough. Patients must feel prepared to use a prosthesis.
Follow-ups are the right time to build confidence and reduce fear.
Patients often worry about pain, control, and daily use. Addressing these concerns early builds trust.
Clear, honest answers prevent anxiety-driven delays later.
Even small improvements should be acknowledged. This helps patients stay motivated.
Progress-focused follow-ups keep hope strong and realistic.
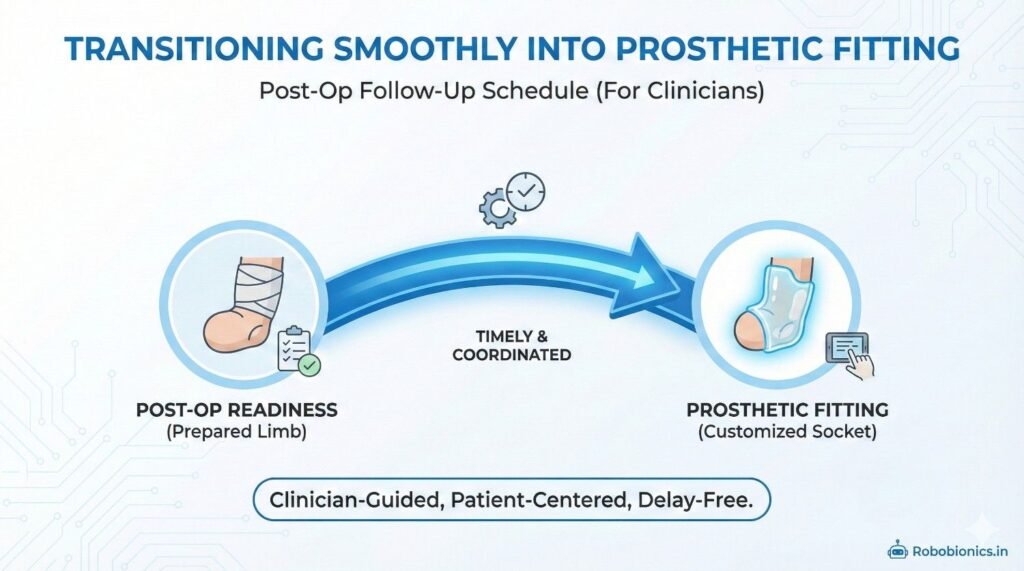
The shift from clinical follow-up to prosthetic fitting is a common delay point.
Clear handover plans prevent patients from feeling lost between teams.
Before fitting, a final readiness update should be shared with the prosthetic team.
This reduces repeated assessments and speeds up the first fitting session.
Clinician involvement should not end at fitting. Early prosthetic use often raises new questions.
Short follow-ups after fitting help catch issues early and protect long-term outcomes.
Great outcomes should not depend on one experienced clinician. Systems ensure consistency across staff.
A repeatable follow-up system reduces errors and delays.
All staff should understand why each follow-up step matters.
When the whole team shares the same goals, care becomes smoother.
No system is perfect forever. Regular reviews help refine timing and communication.
Clinics that improve their systems over time see fewer prosthetic delays year after year.
A written follow-up schedule brings clarity to everyone involved. It reduces guesswork and ensures no stage is skipped.
When clinicians, patients, and prosthetic teams follow the same timeline, delays reduce naturally and outcomes improve steadily.
During this period, the focus remains on wound protection and pain control. Patients should understand how to care for the limb safely.
This is also the time to explain the full recovery journey in simple terms, so expectations are set early and clearly.
The first review checks wound condition and early swelling. Any signs of infection or delayed closure must be addressed quickly.
Clear instructions for the next phase should be given, along with confirmation of the next visit date.
At this stage, the wound should show steady improvement. Swelling trends become more visible.
This visit is ideal for starting or reinforcing limb shaping strategies and preparing the patient for future prosthetic steps.
By now, controlled movement should be encouraged. Clinicians should check basic muscle activity and joint comfort.
Any stiffness or pain should be addressed early to avoid delays during prosthetic training.
This visit focuses on overall readiness. Skin tolerance, limb sensitivity, and volume stability are reviewed together.
A prosthetic referral should already be active by this stage, even if fitting is planned later.
If healing and limb condition are stable, this phase confirms readiness for casting or scanning.
Clear communication with the prosthetic team at this point prevents last-minute delays.
When follow-ups become checklist-only visits, important details get missed.
Each visit should be purposeful and linked to the larger prosthetic goal.
Small issues often grow when ignored. Delaying action on swelling, pain, or skin issues is a common cause of prosthetic delay.
Early escalation saves time, even if it feels cautious at first.
Patients who feel excluded from decisions are less engaged.
Involving them during follow-ups improves compliance and speeds recovery.
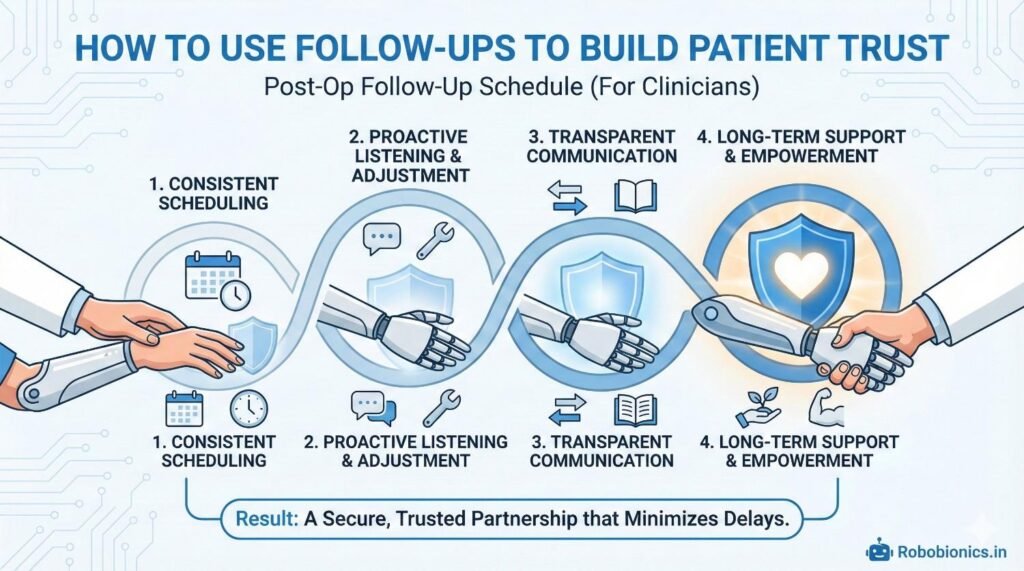
Seeing the same messages repeated across visits reassures patients.
Consistency in advice and timelines strengthens trust in the care process.
Being honest about challenges does not reduce hope. It strengthens credibility.
Patients value clarity more than false reassurance.
Pointing out healing progress helps patients stay positive.
Even small improvements matter when they are acknowledged clearly.
Patients who follow structured post-op care adapt faster to their prosthesis.
They experience fewer fitting issues and better long-term comfort.
Clear systems reduce repeated visits and last-minute changes.
Clinics operate more smoothly when delays are minimized.
When clinicians follow predictable timelines, prosthetic teams respond with better planning and support.
This partnership improves outcomes for everyone involved.
Surgery is a milestone, not the finish line. What follows determines true recovery.
Post-op follow-up is where outcomes are shaped.
Clear schedules outperform experience-based guessing.
Structure brings reliability, even in busy clinical settings.
Clinicians who guide patients with clarity reduce delays naturally.
When follow-up is done with intention, prosthetic care becomes faster, smoother, and more successful.
For trauma amputees, the journey does not begin at the prosthetic clinic. It begins much

Amputation after cancer is not just a surgical event. It is the end of one

When a child loses a limb, the challenge is never only physical. A child’s body

Age changes the body, but it does not take away the need for independence, dignity,